Garrett Teskey, DO1, Wesley Chow, MD2, Abraham Lopez, MD2, Steven Wong, MD2, Steven Gauerke, MD2, Melanie De Shadarevian, DO3 1Scripps Mercy Hospital, Yorba Linda, CA; 2Scripps Mercy Hospital, San Diego, CA; 3valley medical hospital, San Diego, CA Introduction: Emphysematous gastritis is an uncommon condition characterized by the presence of air within the stomach wall, typically attributed to gas-forming microorganisms. This condition carries a high mortality rate, emphasizing the critical importance of prompt diagnosis and treatment to prevent fatal outcomes. Here, we present a remarkably rare case of emphysematous gastritis secondary to advanced gastric adenocarcinoma.
Case Description/
Methods: A 60-year-old male presented to the ED with one week of right upper quadrant pain. He reported several months of severe postprandial cramping pain, exacerbated by fatty or spicy meals, and a 10-15 pound weight loss about one month prior to admission. Initial labs indicated elevated alkaline phosphatase levels, microcytic anemia, and new onset transaminitis, with an R factor of 0.6, suggesting cholestatic injury. Right upper quadrant ultrasound revealed nonspecific gallbladder wall thickening, mild common bile duct dilation and no cholelithiasis. Subsequent MRCP revealed nonspecific gallbladder wall thickening, but no visible intraductal mass or calculi. Soon after, the patient became unresponsive and hemodynamically unstable. The patient was intubated, started on vasopressor support, and transferred to the ICU. Following stabilization, a STAT CT AP with IV contrast was preformed which revealed emphysematous gastritis with a sizable 7.4 x 14.0 cm gas-containing, rim-enhancing perigastric fluid collection. Prompting emergent exploratory laparotomy. Purulent fluid was found in left mid and upper abdomen, accompanied by diffuse inflammation and thickening of the stomach wall as well as a large area of gastric ischemia and necrosis, necessitating a subtotal gastrectomy. Biopsy results demonstrated poorly differentiated gastric carcinoma with signet-ring cells. Discussion: This case presentation is significant as an extensive literature review reveals only four previously documented cases of emphysematous gastritis linked to cancer, with just two associated with gastric adenocarcinoma. Emphysematous gastritis’s rarity and subsequent lethality requires a high level of clinical suspicion for timely diagnosis and intervention. This case highlights the rapid progression of the disease and the consequences of misdiagnosis. Early detection can enable successful medical management, avoiding the necessity for surgery. However, the condition's rarity often complicates diagnosis.
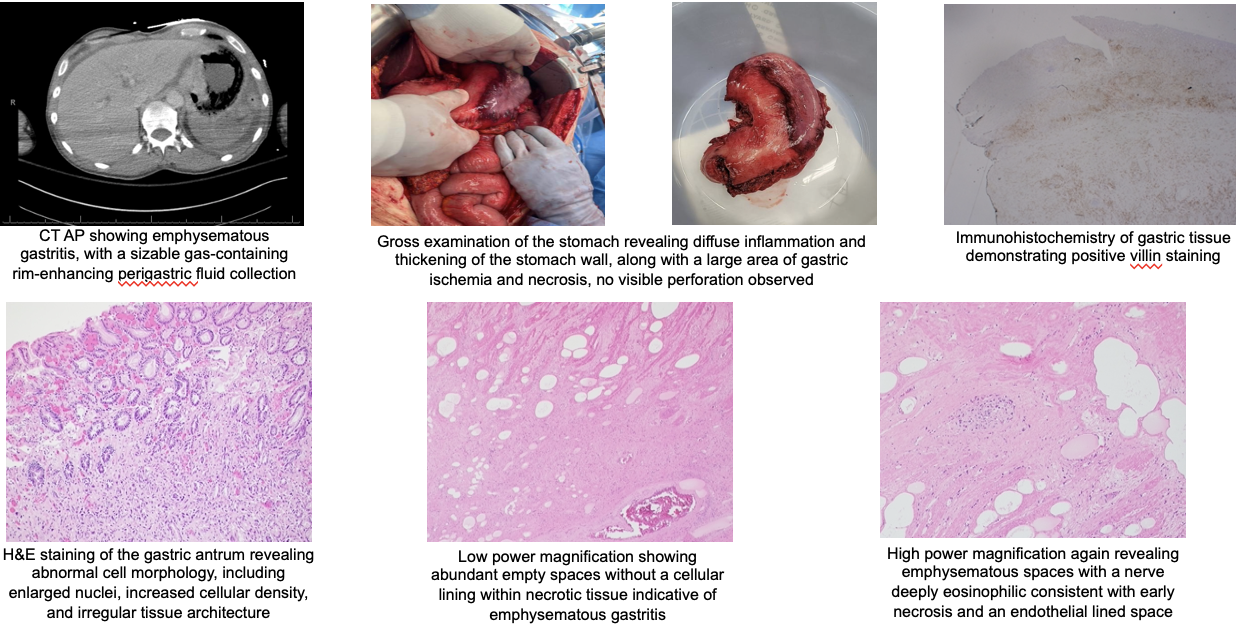
Figure: CT AP showing emphysematous gastritis, with a sizable gas-containing rim-enhancing perigastric fluid collection; Gross examination of the stomach revealing diffuse inflammation and thickening of the stomach wall, along with a large area of gastric ischemia and necrosis, no visible perforation observed; Low power magnification showing abundant empty spaces without a cellular lining within necrotic tissue indicative of emphysematous gastritis.
Disclosures: Garrett Teskey indicated no relevant financial relationships. Wesley Chow indicated no relevant financial relationships. Abraham Lopez indicated no relevant financial relationships. Steven Wong indicated no relevant financial relationships. Steven Gauerke indicated no relevant financial relationships. Melanie De Shadarevian indicated no relevant financial relationships.
Garrett Teskey, DO1, Wesley Chow, MD2, Abraham Lopez, MD2, Steven Wong, MD2, Steven Gauerke, MD2, Melanie De Shadarevian, DO3. P6384 - A Rare Case of Emphysematous Gastritis Precipitated by Advanced Gastric Adenocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.