Viraj Modi, DO1, Omar Jureyda, DO2, Fernando Lugo-Hernandez, MD1, Ebiuwa A. Osula, MD, MS, MBS3, Farrukh Saeed, MD1 1HCA Florida Healthcare, Brandon, FL; 2HCA Florida Healthcare, Tampa, FL; 3HCA Healthcare, Tampa, FL Introduction: Chronic cholecystitis is a subacute condition caused by mechanical or functional dysfunction of emptying of the gallbladder. This long standing inflammation may result in obstruction through gallstone translocation through a fistula, however this has not been reported as solely secondary to reactive changes. We present the case of a 68 year old female who developed a large bowel obstruction secondary to inflammatory changes from chronic cholecystitis.
Case Description/
Methods: A 68 year old female with a history of a noncancerous colon polyp, and no prior surgical history complains of crampy abdominal pain for several months. The pain is described as diffuse, only occasionally triggered by food with associated worsening nonbloody, nonbilious emesis, loose bowel movements and approximately 20 pound weight loss. A CT abdomen showed acute cholecystitis and possible choleduodenal fistula. A dilated small bowel and ascending colon was noted, with a transition point near hepatic flexure. She was started on appropriate antibiotics with surgical and gastrointestinal consultation. Gastrografin enema showed evidence of incomplete obstruction with contrast in ascending colon, however consistent with possible extrinsic inflammatory changes; no fistula was identified. MRCP confirmed cholecystitis, and a colonoscopy to rule out cancerous mass identified a large 30 mm polypoid mass, however pediatric scope was unable to be passed. Pathology from colonic biopsy confirmed reactive changes. She was discharged after tolerating diet, and continued improvement with stool habits over several months with plans for outpatient cholecystectomy. Discussion: Bowel obstruction secondary to cholecystitis often results in a fistulous tract, with gallstone passage blocking the intestinal lumen. In our patient, despite being unable to traverse the obstruction on colonoscopy the CT with enema identified no fistulous tracts between gallbladder and bowel. Biopsy results obtained from colonoscopy noted reactive changes of the colon, and ruled out colon cancer at the hepatic flexure. With biopsy findings suggestive reactive changes, and gallstone effectively being ruled out with imaging studies, the most likely culprit of this patient’s large bowel stenosis is likely chronic inflammation. Post hospitalization, the patient noted symptomatic improvement with an additional 10 days of oral antibiotics and low fat diet to attempt to reduce colic symptoms and plans for outpatient cholecystectomy.
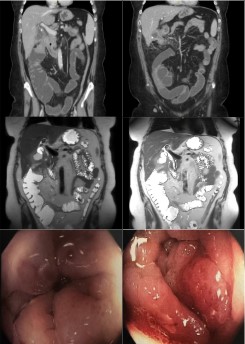
Figure: Top row. CT images showing transition point at hepatic flexure with gallbladder wall thickening and stone within body. Middle row. MRI of abdomen showing gallbladder wall inflammation with large bowel dilatation and left upper quadrant transition point, no fistula noted. Bottom row. Colonoscopy findings of severely stenosed large bowel at the left upper quadrant unable to be traversed.
Disclosures: Viraj Modi indicated no relevant financial relationships. Omar Jureyda indicated no relevant financial relationships. Fernando Lugo-Hernandez indicated no relevant financial relationships. Ebiuwa Osula indicated no relevant financial relationships. Farrukh Saeed indicated no relevant financial relationships.
Viraj Modi, DO1, Omar Jureyda, DO2, Fernando Lugo-Hernandez, MD1, Ebiuwa A. Osula, MD, MS, MBS3, Farrukh Saeed, MD1. P0175 - Chronic Cholecystitis Presenting with Incomplete Large Bowel Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.