P0053 - Multicenter Comparison of Endoscopic Ultrasound-Guided Choledochoduodenostomy versus Gallbladder Drainage for Malignant Biliary Obstruction: A Propensity Score-Matched Study
Brigham and Women's Hospital, Harvard Medical School Boston, MA
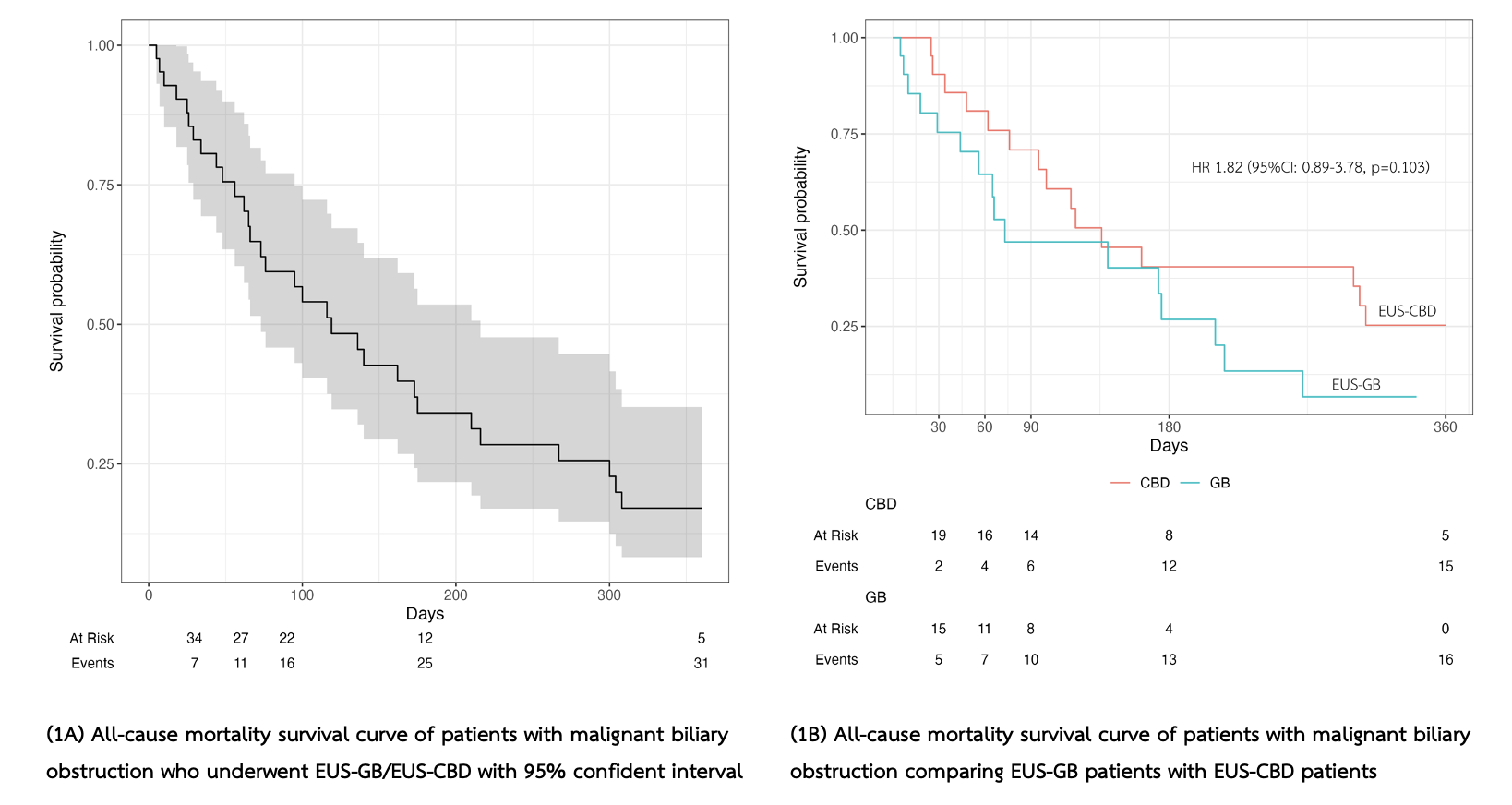
Noppachai Siranart, MD, Steven Steinway, MD Brigham and Women's Hospital, Boston, MA Introduction: Endoscopic ultrasound-guided gallbladder drainage (EUS-GB) is an emerging alternative to choledochoduodenostomy (EUS-CBD) for malignant distal biliary obstruction (MDBO). Previous literature suggests that EUS-GB can be useful as a salvage approach in MDBO in patients when ERCP and EUS-CBD are unsuccessful or not feasible. However, there is a paucity of research on the relative efficacy and safety profiles of EUS-GB versus EUS-CBD as a primary approach for direct access biliary drainage. Methods: We conducted a multicenter, retrospective study of patients undergoing EUS-GB or EUS-CBD for MDBO between January 2015 and October 2024. Primary outcomes were technical and clinical success. Secondary outcomes included procedural time, 6-month reintervention, adverse events (AEs), and all-cause mortality. Propensity score matching (PSM) was used to adjust for baseline differences. Results: Eighty-two patients were included in this study. Of these, 22(26.8%) underwent EUS-GB and 60(73.2%) underwent EUS-CBD (Table 1). Primary outcomes: Technical success was comparable between groups (95.5% vs. 96.7%). EUS-GB was used as salvage in 50% of cases when EUS-CBD was not feasible (n=11), with a 90.9% technical success rate. PSM yielded 21 matched pairs. Clinical success was similar (95.2% EUS-GB vs. 85.7% EUS-CBD, p=0.61). Secondary outcomes: EUS-CBD had significantly lower 6-month reintervention (4.8% vs. 23.8%, p=0.004) and stent-related complications (0% vs. 18.9%). Median time to reintervention was 66(13-181) days. Adverse event rates and all-cause mortality were similar. Median follow-up was 116 days (IQR: 51–300). In the EUS-GB group, pre-procedural cystic duct patency predicted clinical success (94.1%). All-cause mortality was comparable in both groups with HR 1.82 (95%CI: 0.89-3.78). (Figure 1).
Discussion: EUS-GB is a technically effective and clinically comparable alternative to EUS-CDS as upfront strategy for direct access biliary drainage for MDBO after failed ERCP, with significantly fewer re-interventions and stent-related complications. When cystic duct patency is confirmed on imaging, EUS-GB may be considered as a primary approach or salvage strategy for direct access biliary drainage in MDBO after failed ERCP.
Figure: Table 1. Baseline characteristics of included MDBO patients
Figure: Figure 1. Survival analysis showed all-cause mortality was comparable in both groups.
Disclosures: Noppachai Siranart indicated no relevant financial relationships. Steven Steinway indicated no relevant financial relationships.
Noppachai Siranart, MD, Steven Steinway, MD. P0053 - Multicenter Comparison of Endoscopic Ultrasound-Guided Choledochoduodenostomy versus Gallbladder Drainage for Malignant Biliary Obstruction: A Propensity Score-Matched Study, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.