University of Miami Miller School of Medicine at Holy Cross Hospital Fort Lauderdale, FL
Award: ACG Presidential Poster Award
John Coleman, MD1, Akram Ahmad, MD2, Anas Khouri, MD2, Ingrid C.. Landfald, MD3, Tilak Shah, MD2, Gloria Francis, MD4 1University of Miami Miller School of Medicine at Holy Cross Hospital, Fort Lauderdale, FL; 2Cleveland Clinic Florida, Weston, FL; 3Department Of Clinical Anatomy Mazovian Academy, Płock, Poland, Poland, Mazowieckie, Poland; 4Cleveland Clinic Florida, Coral Springs, FL Introduction: Bouveret syndrome is a rare complication of cholelithiasis that occurs when a large gallstone migrates through a bilioenteric fistula, most commonly cholecystoduodenal, and becomes lodged in the duodenum, leading to gastric outlet obstruction.
Case Description/
Methods: We present the case of an 87-year-old female with a history of diabetes and prior hysterectomy who presented with epigastric pain and bilious emesis after a fatty meal. Imaging revealed pneumobilia, gastric outlet obstruction, and a 31 mm obstructing gallstone in the duodenum (Rigler’s triad). Upper endoscopy confirmed a large stone in the duodenal bulb and a visible cholecystoduodenal fistula. Despite the gamut of attempts at endoscopic retrieval including a Roth net, a large snare, rat tooth forceps, suction, and electrohydraulic lithotripsy (EHL), endoscopic retrieval was not successful. The patient subsequently underwent a laparoscopic enterotomy with successful stone extraction via jejunostomy. Cholecystectomy and fistula repair were deferred to minimize operative risk given the patient’s age. She recovered uneventfully and was discharged on postoperative day five. Discussion: This case highlights several key aspects of Bouveret syndrome that would be valuable to clinicians: characteristic signs and symptoms of the syndrome, imaging features, and a description of endoscopic as well as surgical approaches. Endoscopic management is often preferred in elderly or high-risk patients, surgical intervention remains the most definitive treatment following failed endoscopy.
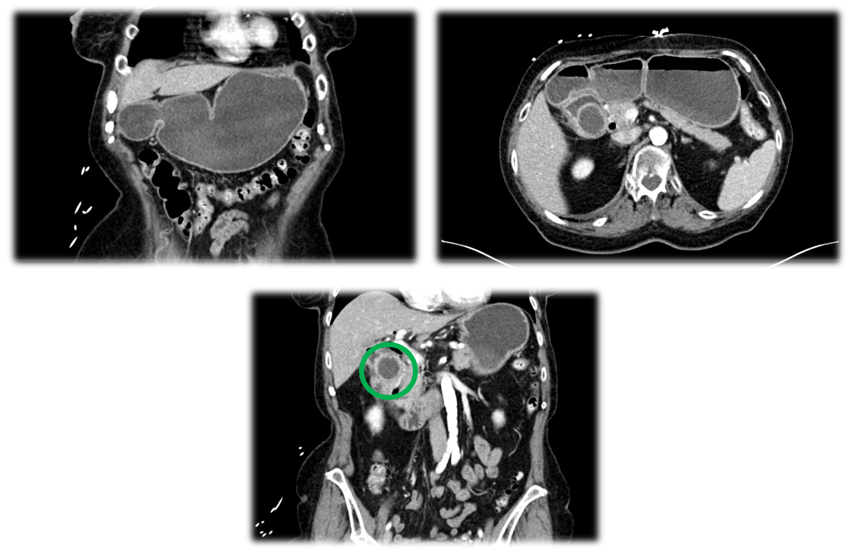
Figure: Figure 1ab. A computerized tomography scan of the abdomen and pelvis with coronal view (top left) and axial view (top right) revealing pneumobilia and cholecystoduodenal fistula in addition to a distended stomach and duodenum secondary to a gallstone measuring approximately 31mm in diameter, causing complete obstruction. Figure 2. A computerized tomography scan of the abdomen and pelvis with coronal view showing large gallstone within the proximal duodenum causing complete intestinal obstruction (green circle).
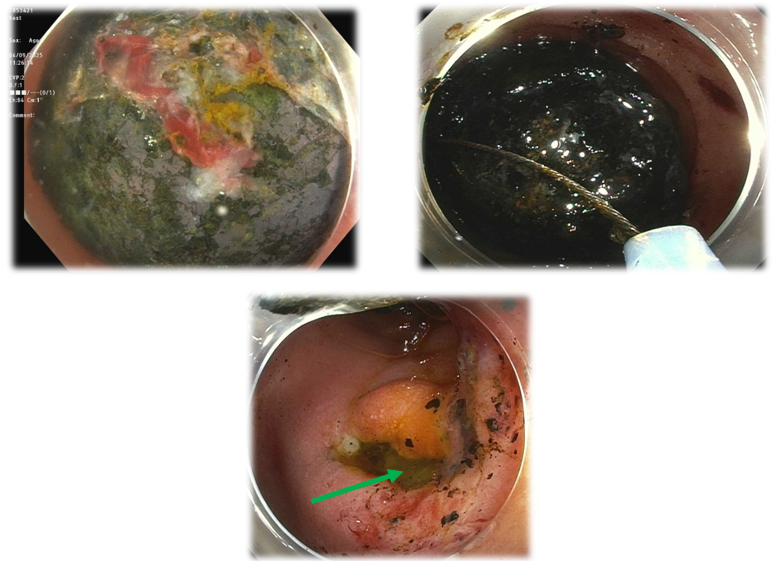
Figure: Figure 3. Direct visualization via endoscopic imaging of large gallstone within the duodenum after unsuccessful EHL procedure (top left). Direct visualization of gallstone in an attempt at snare removal (top right). Figure 4. Endoscopic imaging of cholecystoduodenal fistula with active bilious drainage seen within the duodenal bulb (bottom, green arrow).
Disclosures: John Coleman indicated no relevant financial relationships. Akram Ahmad indicated no relevant financial relationships. Anas Khouri indicated no relevant financial relationships. Ingrid Landfald indicated no relevant financial relationships. Tilak Shah: Steris – Consultant. Gloria Francis indicated no relevant financial relationships.
John Coleman, MD1, Akram Ahmad, MD2, Anas Khouri, MD2, Ingrid C.. Landfald, MD3, Tilak Shah, MD2, Gloria Francis, MD4. P0138 - A Rock in a Hard Place: Endoscopic and Surgical Management of Bouveret Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.