Hobie L. Hughes, DO1, Lauren Healey, DO2, Nathaniel Winstead, MD, MSPH, FACG1, Jonathan Francis, MD1, Matthew Eves, MD1 1Thomas Hospital, Fairhope, AL; 2University of South Alabama, Mobile, AL Introduction: Ascending cholangitis is an acute infection of the biliary tree, typically resulting from biliary obstruction. Common symptoms associated with ascending cholangitis include fevers, jaundice, right upper quadrant abdominal pain, and hypotension and altered mental status in severe cases. The most common causes of biliary obstruction are choledocholithiasis and benign biliary strictures. Malignant biliary strictures are a much less common cause. Cholangiocarcinoma and pancreatic adenocarcinoma are the most common cause of malignant biliary strictures with the most common metastatic cause being colorectal cancer. Biliary obstruction secondary to intraluminal common bile duct (CBD) metastasis of clear-cell renal cell carcinoma (ccRCC) is extremely rare with only a few documented cases as the cause of ascending cholangitis.
Case Description/
Methods: A 92-year-old female with a history of type 2 diabetes mellitus, hypertension, and clear cell renal cell carcinoma status post right nephrectomy in 2011, presented for evaluation of weakness, abdominal pain, and fevers. Initial workup revealed gram-negative bacteremia and elevated liver function tests. A recent magnetic resonance imaging showed a large intraluminal lesion measuring 1.6 x 1.9 x 3.2 cm dilating the CBD with arterial phase enhancement. The patient underwent endoscopic retrograde cholangiopancreatography (ERCP) which showed evidence of an intraluminal mass in the lower third of the CBD with choledocholithiasis past the mass. Partial removal of gallstones was achieved with a biliary sphincterotomy and placement of a covered metal stent. Significant purulence was noted during the ERCP consistent with ascending cholangitis. The intraluminal mass was biopsied with pathology confirming metastatic ccRCC. Discussion: Ascending cholangitis is a clinical syndrome characterized by fever, jaundice, and abdominal pain that develops as a result of stasis and infection in the biliary tract. Cholangitis was first described as a serious and life-threatening illness, however it is now recognized as a disease ranging from mild to life-threatening. Biliary obstruction from metastatic ccRCC is rare, with only a few documented cases as the cause of ascending cholangitis. Along with initiation of antibiotic therapy, ERCP with sphincterotomy and stone extraction is the treatment of choice for the majority of uncomplicated cases. In patients with known prior malignancy presenting with symptoms of cholangitis, metastasis should always be kept on the differential.
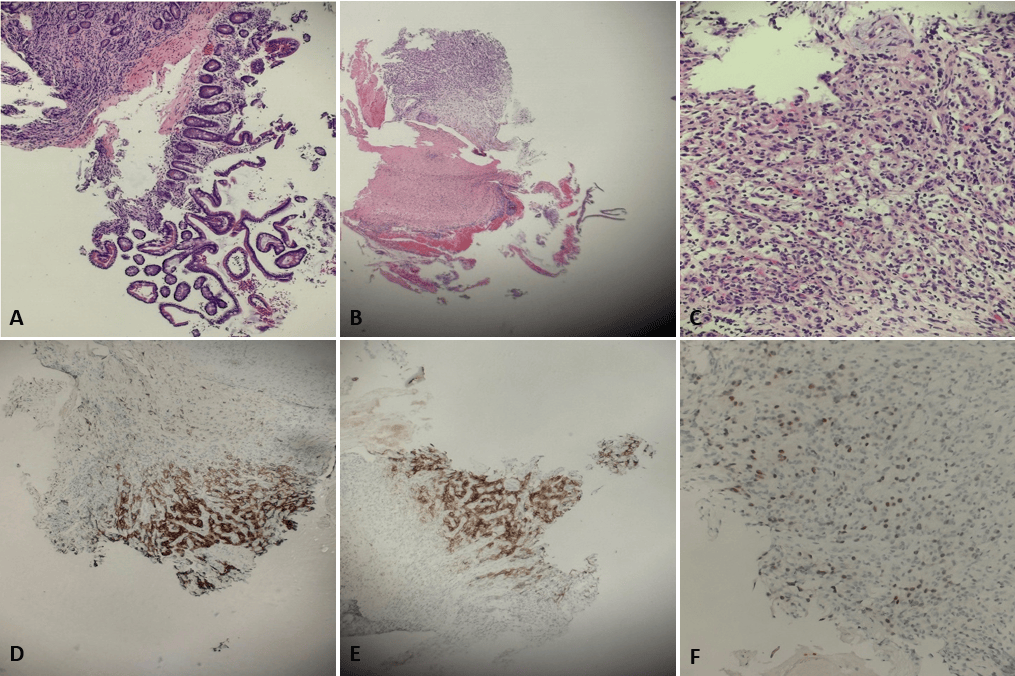
Figure: A: Normal small bowel mucosa. B: Ulcerated small bowel mucosa at bottom of image with underlying atypical cells at top of image. C: High-powered view showing atypical cells with cytoplasmic clearing and low-grade nuclei. D: Pax8 immunostaining positive meaning likely renal origin. E: Pankeratin positive confirming epithelial origin. F: CD10 positive consistent with clear-cell renal cell carcinoma.
Disclosures: Hobie Hughes indicated no relevant financial relationships. Lauren Healey indicated no relevant financial relationships. Nathaniel Winstead indicated no relevant financial relationships. Jonathan Francis indicated no relevant financial relationships. Matthew Eves indicated no relevant financial relationships.
Hobie L. Hughes, DO1, Lauren Healey, DO2, Nathaniel Winstead, MD, MSPH, FACG1, Jonathan Francis, MD1, Matthew Eves, MD1. P0132 - A Clear Obstruction: Metastatic Clear Cell Renal Cell Carcinoma Masquerading as a Common Bile Duct Mass, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")