Karteek MI. Chennupati, MD, MS1, Zeeshan Ramzan, MD2, Rebecca Whitmer, MD3 1Texas Health Resources, FW, Fort Worth, TX; 2Texas Health Physician Group, Keller, TX; 3Texas Health Harris Methodist, Fort Worth, TX Introduction: Ganglioneuromas are benign tumors derived from mature ganglion cells, often involving sympathetic or parasympathetic nerve fibers. They are typically found in the retroperitoneum, adrenal glands, or along sympathetic nerve trunks. Pancreatic involvement is extremely rare with very few cases reported in medical literature. This case report describes a 21-year-old male presenting with abdominal pain and found to have a pancreatic mass.
Case Description/
Methods: A 21-year-old male with no significant past medical history presented with a 12-hour history of periumbilical abdominal pain with radiation to the right upper quadrant. The pain was described as dull with no clear relation to oral intake or body position. The patient reported occasional nausea and early satiety with physical examination only remarkable for mild tenderness in the upper mid-abdomen. Blood work including complete blood count, liver function tests, and pancreatic enzymes were all within normal limits. Initial abdominal ultrasound was inconclusive, prompting further imaging studies. A contrast-enhanced computed tomography scan of the abdomen revealed a well-defined mass in the pancreatic head without evidence of biliary obstruction or pancreatic duct dilation (Figure 1). Magnetic resonance cholangiopancreatography was performed confirming presence of a well-defined heterogeneous mass measuring 5.1 cm x 2.8 cm x 6 cm along the superior margin of the pancreatic head. An endoscopic ultrasound for fine needle aspiration of the mass was done with cytology consistent with ganglioneuroma (Figure 2). The patient was discharged with plans for outpatient hepato-biliary surgery follow up, as well as genetic testing to rule out associated syndromes. Discussion: Pancreatic ganglioneuroma is exceedingly rare, with only a few cases reported in the literature. The clinical presentation is often nonspecific and usually asymptomatic until it reaches a size large enough to cause symptoms related to mass effect like abdominal pain, nausea, vomiting, and jaundice. Imaging studies, including CT and MRI, are helpful in diagnosis, as ganglioneuromas often present as well-defined, non-calcified masses with a characteristic imaging profile. Surgical resection is the gold standard treatment and prognosis is excellent with no recurrence in a vast majority of cases. Further studies should be performed to check for genetic syndromes including Neurofibromatosis 1 (NF1), Multiple Endocrine Neoplasia Type 2B (MEN2B) and Von Hippel Lindau (VHL).
Figure: Figure 1: Image of pancreatic mass (*) on CT abdomen/pelvis with IV contrast. Fine needle aspiration of mass revealed ganglioneuroma.
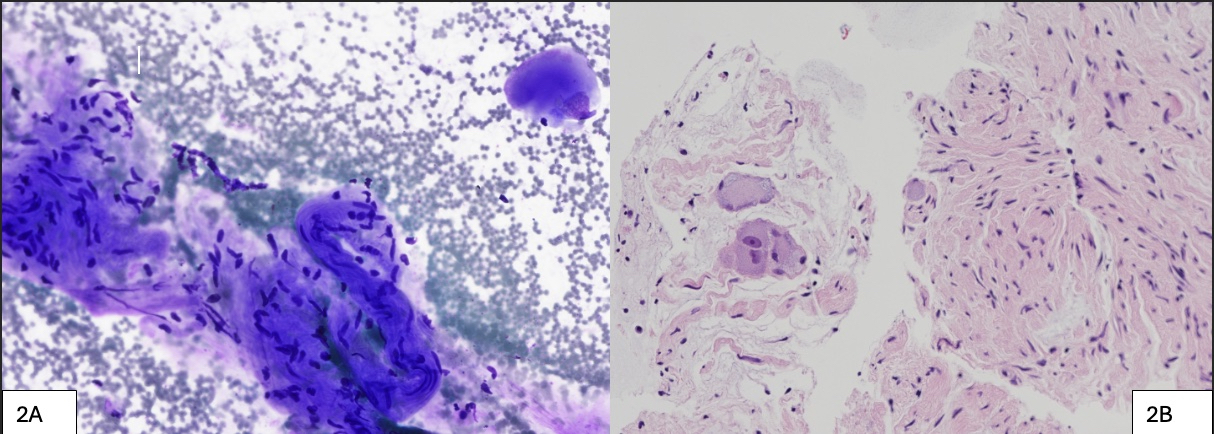
Figure: Figure 2 (A): Fine needle aspiration (FNA) smear, Diff-Quik stain, 200X, showing a ganglion cell in the upper right, with a large nucleus and abundant cytoplasm, as well as aggregates of Schwann cells with uniform spindled nuclei at bottom and left. Figure 2 (B) showing cell block section, H&E stain, 200X, showing a cluster of ganglion cells at left, including one binucleate ganglion cell (a hallmark of ganglioneuroma), along with whorled spindled Schwann cell nuclei. No mitotic figures or necrosis was present.
Disclosures: Karteek Chennupati indicated no relevant financial relationships. Zeeshan Ramzan indicated no relevant financial relationships. Rebecca Whitmer indicated no relevant financial relationships.
Karteek MI. Chennupati, MD, MS1, Zeeshan Ramzan, MD2, Rebecca Whitmer, MD3. P0128 - Unmasking the Silent Giant: Ganglioneuroma of the Pancreatic Head, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")