MedStar Health-Georgetown/Washington Hospital Center Washington, DC
Qusai Al Zureikat, MD1, Stanley Pietrak, MD2 1MedStar Health-Georgetown/Washington Hospital Center, Washington, DC; 2MedStar Georgetown University Hospital, Washington, DC Introduction: Migration of embolization coils is a rare but serious complication following gastroduodenal artery (GDA) embolization. We present a case of recurrent biliary obstruction and bilioduodenal fistula due to migrated coils, requiring multiple interventions.
Case Description/
Methods: A 67-year-old female with a history of GDA coil embolization secondary to bleeding duodenal abscess presented with one week of abdominal pain. Labs revealed total bilirubin 5.1 mg/dL, direct bilirubin 4.0 mg/dL, AST 207 U/L, ALT 122 U/L, and ALP 673 U/L. MRCP showed intrahepatic and extrahepatic biliary dilation with a large CBD filling defect. ERCP revealed a coil eroding into the duodenal sweep with surrounding inflammation. Deep biliary access was unsuccessful due to extravasation of contrast into the duodenum. ERCP was aborted, and percutaneous transhepatic cholangiography with cholangioscopy was performed, placing a left external biliary drain.
Repeat cholangioscopy 3 weeks later confirmed coil protrusion into the CBD and duodenum. A segment was removed using SpyGlass and forceps, and an internal-external drain was placed. This was later converted to an external drain and removed. The patient re-presented with fatigue, diarrhea, and worsening cholestasis. MRCP showed a 4.2 x 1.4 cm hypointense filling defect occluding the CBD. Ultrasound confirmed obstruction. Repeat ERCP revealed migrated coils within a bilio-enteric fistula. Deep CBD cannulation was achieved using a guidewire and sphincterotome. A 9 mm balloon sweep cleared sludge and stones, and two stents were placed: one via the fistula and one across the ampulla. Labs improved (bilirubin 2.0 mg/dL, AST 82 U/L, ALT 96 U/L, ALP 540 U/L). Four months later, liver tests normalized further. ERCP showed persistent biliary dilation and contrast drainage via the fistula. Both stents were removed, and a temporary 10 mm x 6 cm biliary stent was placed, with plans for removal in 2-3 months. Discussion: Coil migration after gastroduodenal artery embolization is a rare but significant complication that can lead to biliary obstruction, cholangitis, and fistula formation. Migrated coils may act as a nidus for stone formation or directly obstruct the bile duct, causing recurrent symptoms. Prompt recognition is essential, particularly in patients with a history of embolization who present with unexplained biliary issues. Management is often multidisciplinary, with endoscopic removal as first-line therapy and percutaneous or surgical approaches reserved for more complex cases.
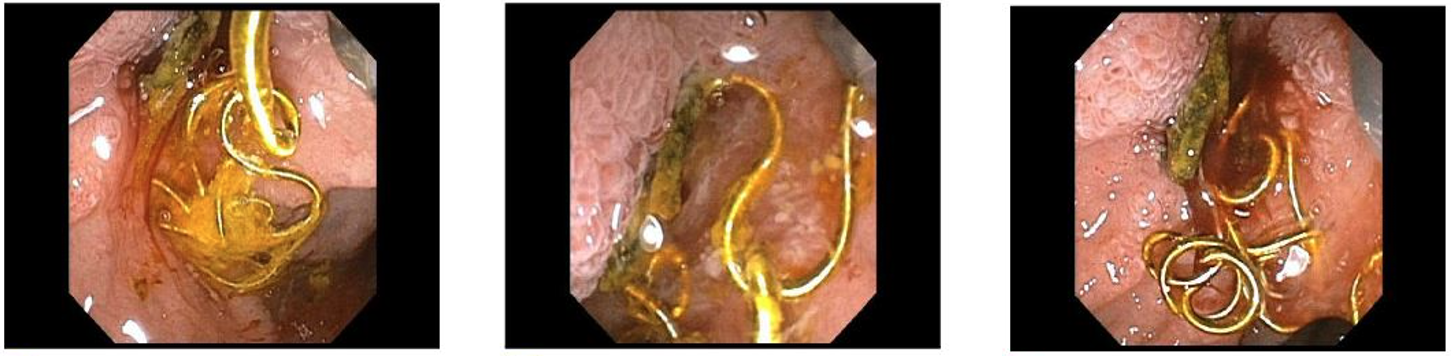
Figure: Migrated embolization coils within biliary tract
Disclosures: Qusai Al Zureikat indicated no relevant financial relationships. Stanley Pietrak indicated no relevant financial relationships.
Qusai Al Zureikat, MD1, Stanley Pietrak, MD2. P0124 - Unraveling the Coil: Endoscopic Rescue of Biliary Obstruction From Migrated Embolization Coils, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")