Solomon Anighoro, MBBS1, Raja Chandra Chakinala, MD2, Rewanth Katamreddy, MD2, Chaitanya K. Chandrala, MD2, Michael Georgetson, MD, FACG2 1Guthrie Robert Packer Hospital, Sayre, PA; 2Guthrie Robert Packer Hospital, Department of Gastroenterology, Sayre, PA Introduction: Gallbladder cancer is the most common biliary tract malignancy; however, pure squamous cell carcinoma (SCC) represents only 1%, with adenosquamous types comprising 4% [1]. Pure SCC is particularly aggressive, often presenting with advanced local invasion and a high likelihood of positive margins despite radical surgery [1–3]. Unlike adenocarcinoma, its etiopathogenesis remains unclear, though chronic cholecystitis, gallstones, and infections have been implicated. Recent molecular profiling efforts may help identify therapeutic targets [2]. We report a case of primary pure SCC of the gallbladder and discuss clinical presentation, diagnostic approach, and management in the context of current literature.
Case Description/
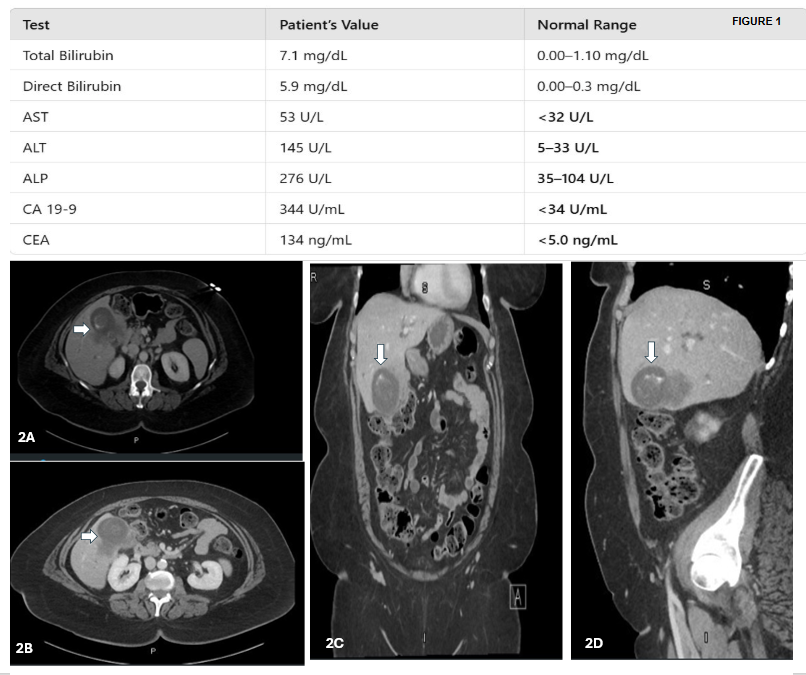
Methods: A 60-year-old woman with type 2 diabetes presented with abdominal bloating, jaundice, and dark urine. She had no history of smoking, alcohol use, or family history of liver disease. Labs showed elevated liver enzymes and bilirubin (Figure 1); viral hepatitis panel was negative.
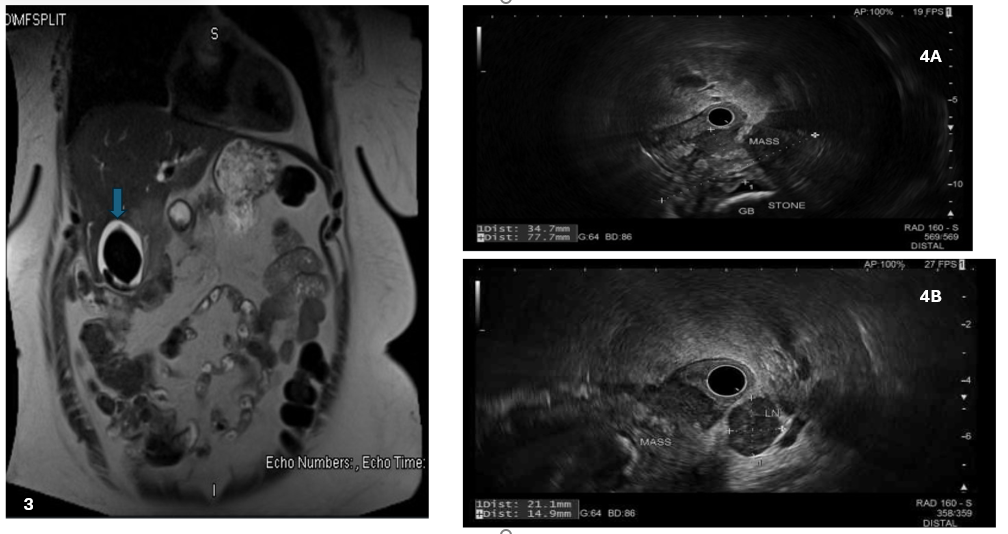
CT imaging revealed a distended gallbladder with cholelithiasis, wall thickening, and extension into hepatic parenchyma, along with regional lymphadenopathy (Figure 2). MRI showed a 6.7 cm enhancing mass with intrahepatic biliary dilation (Figure 3). EGD was unremarkable, but EUS identified a gallbladder mass and suspicious lymph nodes (Figure 4). ERCP showed strictures and biliary dilation. FNA of hepatic and nodal lesions confirmed squamous cell carcinoma. IHC positive for CAM 5.2, CK5/6 and p40 and negative for CA 19.9, chromogranin, TTF-1, Napsin A, GATA3, PAX8 and WT1. Staging was T3N2M0 (Stage IVb).
She was started on systemic therapy with gemcitabine, cisplatin, and durvalumab. A surgical evaluation was planned pending PET-CT results to assess for metastasis.
Discussion: SCC of the gallbladder presents similarly to adenocarcinoma, with symptoms such as right upper quadrant pain and obstructive jaundice. Imaging aids in evaluating disease extent but lacks specificity for histologic subtype. Diagnosis requires histopathological confirmation, and in this case, the absence of glandular components confirmed pure SCC. This aligns with previously reported cases [4]. Pure SCC of the gallbladder is a rare, aggressive malignancy with poor prognosis. Diagnosis relies on pathology, and treatment typically follows protocols for adenocarcinoma. Surgical resection with negative margins remains key, though recurrence rates are high. Emerging molecular targets may inform future therapies.
Figure: Figure 1. Initial labs showing cholestatic pattern of elevated liver enzymes with elevated bilirubin. Figure 2. CT scan showing dilated gallbladder (blue arrows) with cholelithiasis and wall thickening and indistinct areas of decreased attenuation extending from the gallbladder into the gallbladder fossa of the hepatic parenchyma.
Figure: Figure 3. MRI showing enhancing mass in the gall bladder fossa of the liver and EUS findings.
Figure 4. Mass and enlarged malignant looking regional lymph node
Disclosures: Solomon Anighoro indicated no relevant financial relationships. Raja Chandra Chakinala indicated no relevant financial relationships. Rewanth Katamreddy indicated no relevant financial relationships. Chaitanya K. Chandrala indicated no relevant financial relationships. Michael Georgetson indicated no relevant financial relationships.
Solomon Anighoro, MBBS1, Raja Chandra Chakinala, MD2, Rewanth Katamreddy, MD2, Chaitanya K. Chandrala, MD2, Michael Georgetson, MD, FACG2. P0222 - Squamous Cell Carcinoma of the Gallbladder: An Unusual Histopathological Entity, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.