Tala B. Shahin, MD, Rahul Pannala, MD Mayo Clinic, Phoenix, AZ Introduction: Synovial sarcoma is a rare, aggressive soft tissue malignancy that most commonly arises in the extremities of adults. Metastasis commonly involves the lungs, lymph nodes, and, less frequently, bone. Involvement of the pancreas is extremely rare and scarcely reported in the literature. Here, we report an unusual case of metastatic monophasic synovial sarcoma to the pancreas.
Case Description/
Methods: A 40-year-old male with a history of monophasic synovial sarcoma of the right thigh with metastasis to the lung presented with abdominal discomfort, constipation, and bloating. CT abdomen and pelvis demonstrated multiple cystic lesions in the pancreas body and tail with the largest cyst measuring 1.3cm. There were no solid masses and the pancreatic duct and parenchyma were otherwise normal. On endoscopic ultrasound examination, there were multiple, scattered unilocular cystic lesions in the pancreatic body and tail in a background of normal appearing pancreatic parenchyma and ductal caliber. The sonographic appearance of the cyst was atypical, with subtle irregular, mural thickening, possibly representing central necrosis. Fine needle aspiration was performed, confirming presence of metastatic synovial carcinoma. Sarcoma-directed therapy was reinstituted. A repeat CT scan performed 2 months after the procedure showed no interval growth in the size of the cystic lesions, or evidence of new metastases. Discussion: Pancreatic metastases are uncommon and account for approximately 2% of all pancreatic malignancies. When present, they most frequently originate from renal cell carcinoma, lung carcinoma, breast carcinoma, or melanoma. Metastasis of synovial sarcoma to the pancreas is exceptionally rare, with only a few cases reported in the literature. In this case, the patient presented with nonspecific gastrointestinal symptoms including abdominal discomfort, bloating, and constipation in the setting of known monophasic synovial sarcoma. The radiographic and sonographic features of his pancreatic cystic lesions were atypical for primary pancreatic neoplasms, particularly due to the multiplicity of lesions and absence of a dominant cystic mass. This case underscores the need to include metastatic disease in the differential diagnosis of pancreatic cystic lesions, especially in individuals with a prior history of sarcoma.
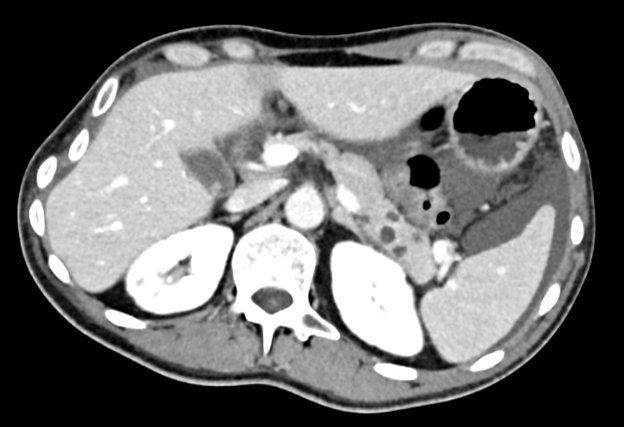
Figure: Figure 1: CT abdomen and pelvis demonstrating multiple cystic lesions of the pancreas body and tail.
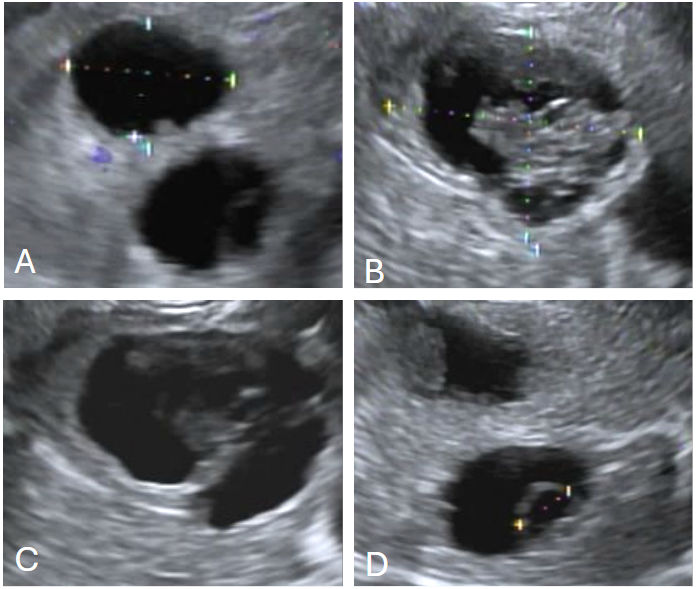
Figure: Figure 2: (Images A-D). Multiple cystic lesions of the pancreatic body and tail, with largest measuring 1.3 cm
Disclosures: Tala Shahin indicated no relevant financial relationships. Rahul Pannala: HCL Technologies – Consultant. Nestlé Health Science – Consultant.
Tala B. Shahin, MD, Rahul Pannala, MD. P0217 - Not Your Usual Pancreatic Cysts: Metastatic Synovial Sarcoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.