Varshita Goduguchinta, DO1, Raahi Patel, DO2, Hardeep Ahdi, MD1, Nabiha Haider, DO1, Amer Alsamman, MD2, Ammar Hassan, DO3 1Franciscan Health, Olympia Fields, IL; 2Franciscan Health Olympia Fields, Olympia Fields, IL; 3Franciscan Health, Munster, IN Introduction: Mirizzi Syndrome (MS) is a rare and often under-recognized condition characterized by extrinsic compression of the common hepatic duct (CHD) or common bile duct (CBD) due to an impacted gallstone in the cystic duct or Hartmann’s pouch. The clinical presentation frequently overlaps with other hepatobiliary conditions, which can lead to delayed recognition. This case series highlights our institutional experience in managing MS, emphasizing the pivotal role of endoscopic intervention in diagnosis and treatment.
Case Description/
Methods: Case 1: A 42-year-old female presented with RUQ abdominal pain. CT showed cholelithiasis and choledocholithiasis with CBD measuring 1.3cm. The patient was afebrile. Labs showed Tbili 2.2mg/dL, ALP 154U/L, AST 383U/L, and ALT 525U/L. No leukocytosis. Lipase 23U/L. MRCP confirmed choledocholithiasis with biliary dilation up to 8mm. ERCP with SpyGlass with cholangioscopy revealed high-grade mid-CBD stricture at the cystic duct level caused by a large, impacted calcified stone consistent with MS. Stone fragmentation and clearance were achieved with a SpyBasket, followed by deployment of a fully covered 10mm×80mm LAMS to facilitate biliary drainage. The patient underwent cholecystectomy the following day. Case 2: A 66-year-old male presented with sudden onset of post-prandial diffuse abdominal pain. On arrival, he had a low-grade fever and HR 120s. Labs showed WBC 18.4 10*3/uL, lactate 3.66mmol/L, AST 144U/L, ALT 103U/L, ALP 156U/L, and Tbili of 1.5mg/dL. RUQ U/S and MRCP demonstrated cholelithiasis without cholecystitis or CBD dilation. An EUS revealed a distended gallbladder with a thickened wall, suggestive of cholecystitis, and multiple hyperechoic clustered stones within the gallbladder neck and cystic duct, pressing on the CHD, suggestive of MS. No ERCP was performed given the lack of stricture, CBD stones, and normal bilirubin. The patient underwent a successful cholecystectomy with complete resolution of symptoms and normalization of labs.
Discussion: These cases exemplify the diverse presentations and management pathways of MS. Both cases showed chronic cholecystitis changes with cholelithiasis post-cholecystectomy. Although rare, MS should be considered in patients with elevated liver enzymes, obstructive jaundice, and gallstones. Early detection using advanced endoscopic techniques such as cholangioscopy and EUS is invaluable in directly visualizing the biliary tree, facilitating both diagnosis and the need for cholecystectomy in the right clinical context.
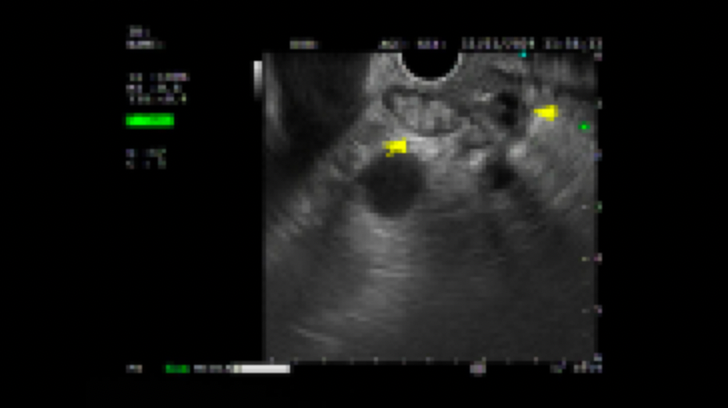
Figure: EUS image showing gallstones with a collapsed wall and prominent hepatic duct concerning for Mirizzi Syndrome
Disclosures: Varshita Goduguchinta indicated no relevant financial relationships. Raahi Patel indicated no relevant financial relationships. Hardeep Ahdi indicated no relevant financial relationships. Nabiha Haider indicated no relevant financial relationships. Amer Alsamman indicated no relevant financial relationships. Ammar Hassan indicated no relevant financial relationships.
Varshita Goduguchinta, DO1, Raahi Patel, DO2, Hardeep Ahdi, MD1, Nabiha Haider, DO1, Amer Alsamman, MD2, Ammar Hassan, DO3. P0214 - Mirizzi on the "Rize": A Case Series on the Endoscopic Management and Outcomes in Mirizzi Syndrome From a Community Hospital System, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")