Johns Hopkins University School of Medicine Baltimore, MD
Vatsal Makhija, 1, Zachariah Foda, MD, PhD2, Anna Stathopoulos, MD, MPHTM2, Keerti Boyapati, BS3 1Jawaharlal Nehru Medical College, Belagavi, India, New Delhi, Delhi, India; 2Johns Hopkins University School of Medicine, Baltimore, MD; 3Johns Hopkins School of Medicine, Baltimore, MD Introduction: Adenomatous polyposis greatly increases the risk of colorectal cancer (CRC) and presents with different genetic etiologies and clinical characteristics. Some polyposis syndromes are inherited, such as Familial Adenomatous Polyposis (FAP) or its milder variant attenuated FAP (aFAP), with a pathogenic variation in the APC gene, and MUTYH-Associated Polyposis (MAP) with a biallelic mutation in the MUTYH gene. Others develop polyposis without a detectable germline mutation as Colonic Polyposis of Unknown Etiology (CPUE).
Current guidelines recommend intensive screening for individuals with colonic polyposis. While FAP patients are at increased risk for extraintestinal cancers, such as thyroid cancer, while MAP and CPUE patients are not.
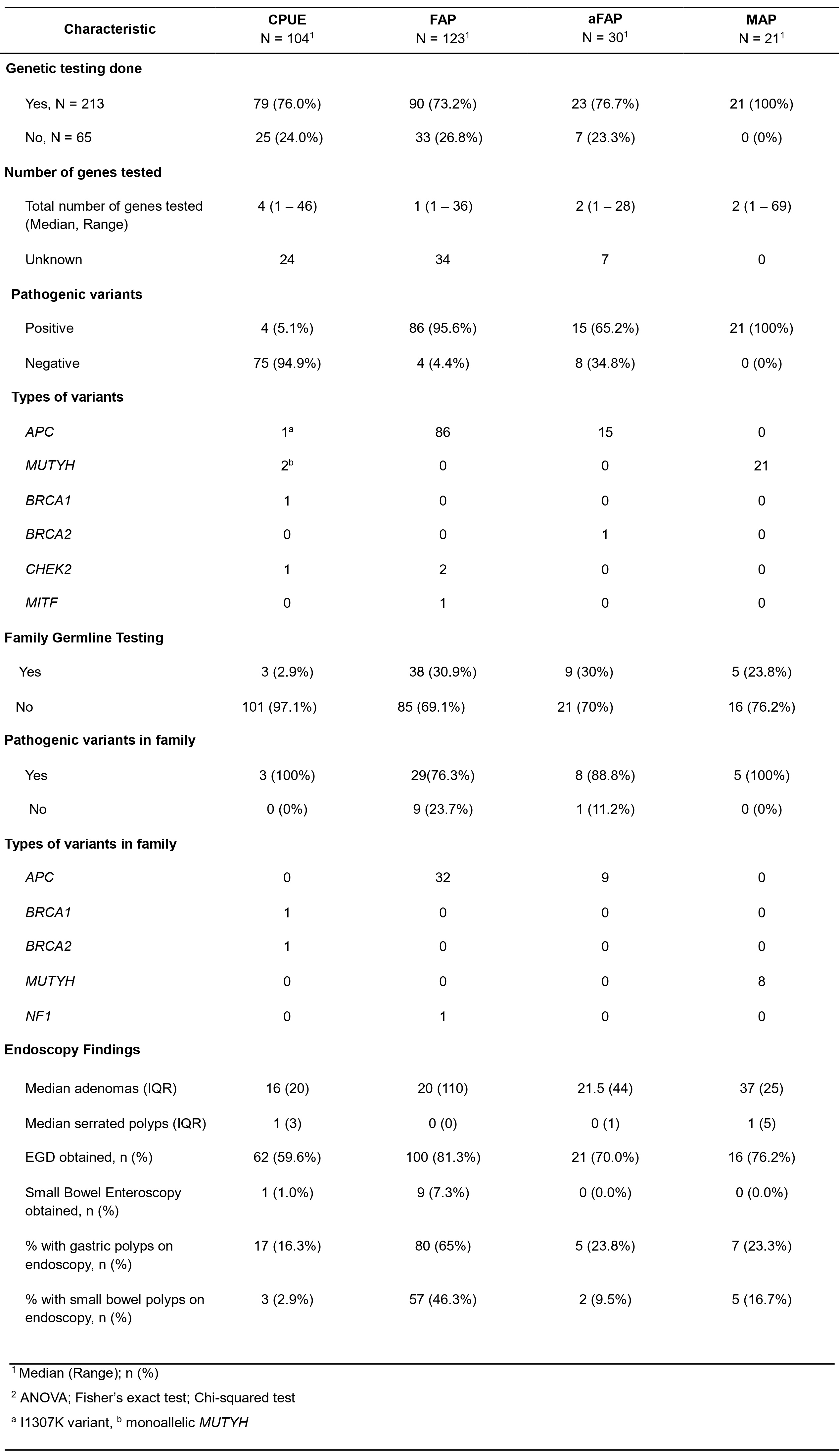
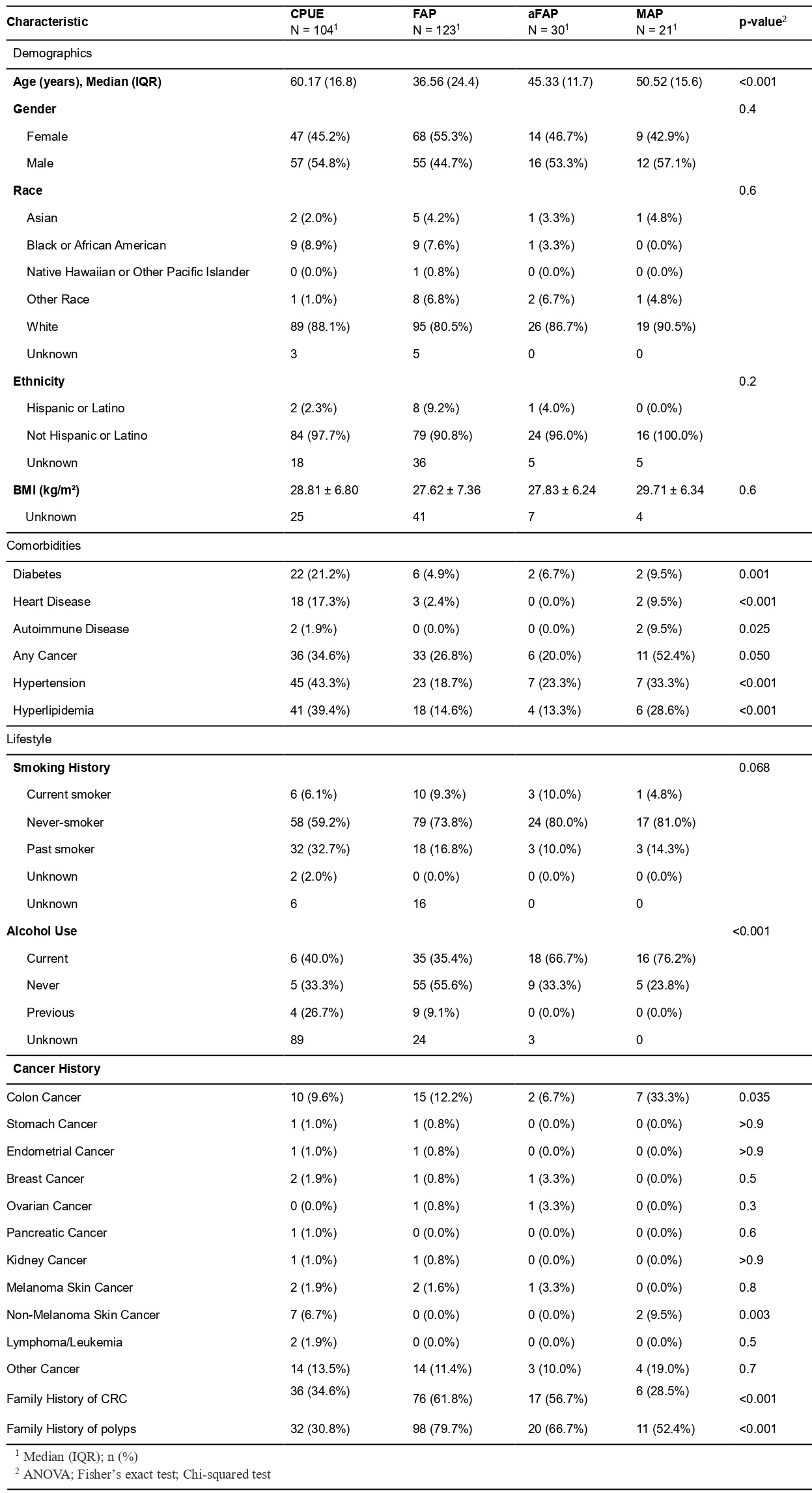
This single-center retrospective study aims to compare the clinical presentations of CPUE, FAP, aFAP, and MAP to guide management for effective CRC prevention. Methods: 278 patients were identified from a research registry at an academic tertiary care center in between 1973 and 2025. Demographic data, genetic testing, and endoscopic findings were collected from retrospective chart review. Descriptive statistics were used to compare individuals across the groups. Significance was determined with Fisher's exact test, ANOVA, Chi square test. Results: 140 (50.4%) of 278 patients were male. Median (IQR) age was 49.62 (27.85) years and significantly higher in the CPUE group (p < 0.001) (Table 1). White individuals were overrepresented across all groups (82.37%). Comorbidities such as diabetes, hypertension, and heart disease were more likely in CPUE. 213 (76.6%) patients had genetic testing done out of which 126 (59.1%) had at least one pathogenic variation. The median and range for genes tested were 4 (1 – 46) for CPUE, 1 (1 – 36) for FAP, 2 (1-28) for aFAP, and 2 (1 – 69) for MAP. FAP had the highest median adenoma count (37) and percentage of gastric (65%) and small bowel polyps (46.3%) whereas CPUE had the lowest measures (16, 16.3%, and 2.9%). Discussion: This analysis identified that despite similar colorectal phenotype, CPUE patients were older with a higher burden of comorbidities, than individuals with genetic polyposes. Endoscopic findings were variable, with FAP having the highest upper gastrointestinal involvement and CPUE having the least. These finding suggest that on top of being a risk factor for CRC, metabolic syndrome may be a risk factor for colonic polyposis.
Figure: Table 1. Baseline Characteristics by Polyposis Type
Figure: Table 2: Genetic Analysis and Endoscopic Findings
Disclosures: Vatsal Makhija indicated no relevant financial relationships. Zachariah Foda: Delfi Diagnostics – Consultant, Intellectual Property/Patents, Royalties. Anna Stathopoulos indicated no relevant financial relationships. Keerti Boyapati indicated no relevant financial relationships.
Vatsal Makhija, 1, Zachariah Foda, MD, PhD2, Anna Stathopoulos, MD, MPHTM2, Keerti Boyapati, BS3. P0291 - Retrospective Analysis of Demographics and Clinical Characteristics of Adenomatous Polyposes, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.