
Sunday Poster Session
Category: Colon

 photo")
Sena Saygili, BS (she/her/hers)
University of Texas Medical Branch, John Sealy School of Medicine
Galveston, TX
A 20-year-old male with history of well controlled HIV on antiretroviral therapy presented to the gastroenterology clinic with a 5-month history of constipation characterized by infrequent, difficult to pass bowel movements, incomplete evacuation, and intermittent hematochezia. The patient denied weight loss, fevers, or nocturnal symptoms and had no significant past medical or surgical history. Dietary history revealed a low-fiber, high-carbohydrate intake. Physical exam was unremarkable. He was initially managed conservatively with polyethylene glycol, methylcellulose, hydration, and dietary modifications for suspected IBS-C. Due to persistent rectal bleeding, a colonoscopy was performed, revealing a 12mm flat rectal lesion concerning for adenoma or condyloma. The polyp was lifted with saline and en-bloc endoscopic mucosal resection was performed. Histopathology demonstrated rectal mucosa with gastric heterotopia. No adenomatous change or dysplasia was identified.
Discussion:
Rectal gastric heterotopia is a rare but important differential for unexplained rectal bleeding in young patients. It may lead to symptoms such as local irritation, ulceration, or bleeding from acid secretion by ectopic parietal cells. This case highlights the diagnostic value of colonoscopy in young patients with persistent bleeding, particularly in the immunocompromised, given its broad differential. Histologic evaluation is necessary, as endoscopic appearance may mimic other lesions. While GH is typically benign, surveillance may be considered if symptoms persist or dysplasia develops. This case emphasizes the importance of maintaining a broad differential when evaluating persistent rectal bleeding in young adults. Rectal gastric heterotopia, although rare, should be considered once more common causes are excluded. Colonoscopic evaluation and histopathologic confirmation are essential for accurate diagnosis and management.
Figure: Figure 1. Colonoscopy shows one 12 mm polyp in the rectum, removed with mucosal resection.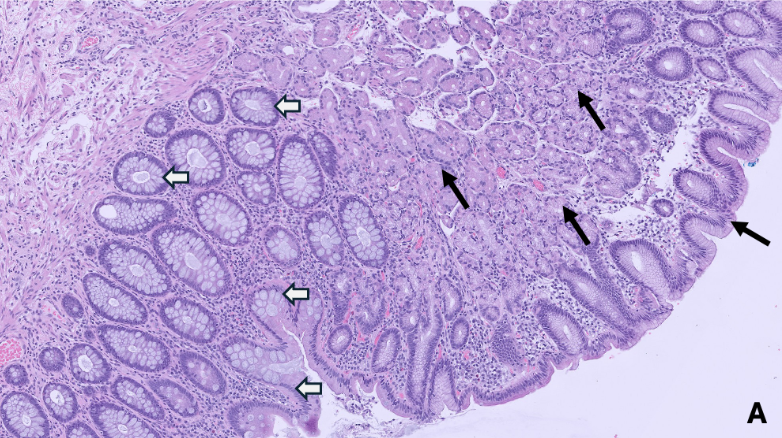
Figure: Figure 2. Rectal polypectomy shows gastric oxyntic type mucosa (black arrow) in rectal mucosal polyp (white arrow) (100x).
Disclosures:
Sena Saygili indicated no relevant financial relationships.
Rebecca Sullivan indicated no relevant financial relationships.
Jing He indicated no relevant financial relationships.
Sreeram Parupudi indicated no relevant financial relationships.
Valerie Quach indicated no relevant financial relationships.
Sena Saygili, BS1, Rebecca C. Sullivan, MD2, Jing He, MD2, Sreeram Parupudi, MD2, Valerie Quach, BS3. P0378 - Atypical Polypoidal Lesion Due to Rectal Gastric Heterotopia Presenting as Hematochezia in a Young Adult, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.