
Sunday Poster Session
Category: Colon
Lorraine I. Chong Tai, MD (she/her/hers)
Broward Health Medical Center
Allentown, PA
Signet ring cell carcinoma (SRCC) of the colon remains one of the rarest forms of colon cancer with an overall poor prognosis. Superior mesenteric artery (SMA) syndrome is an uncommon cause of duodenal obstruction, typically resulting from significant weight loss and loss of the mesenteric fat.
Case Description/
Methods:
A 22 year old female with no history presented for one month of abdominal pain, nausea, vomiting and unintentional weight loss of 30 pounds in 3 months. Computer Tomography (CT) of the abdomen showed a large mass along the inferior aspect of the pancreas and third portion of the duodenum encasing the SMA (Figure 1). Laboratory studies showed a positive fecal occult blood test (FOBT) with elevated tumor markers including, CEA, CA 125 and CA 19-9. A diagnostic laparoscopy revealed a large mass coming out from the transverse colon and attached to the anterior abdominal wall, extending down to the 4th part of duodenum. The mass infiltrated the root of mesentery and the mesenteric vessels with multiple lymph nodes around the mesenteric vessels. Biopsies revealed Signet cell adenocarcinoma of the colon (Figure 2). Immunohistochemical stains for CK20, CDX-2, and E-cadherin were positive. Colonoscopy biopsies confirmed Signet cell adenocarcinoma of the colon. Prior to discharge a chemo port was placed and she underwent initiation of chemotherapy with FOLFOX (Folinic acid, Fluorouracil, and Oxaliplatin) with plans for surgical resection in the future.
Discussion:
The coexistence of SRCC of the colon and SMA syndrome is exceedingly rare and presents a unique diagnostic and therapeutic challenge. Our patient exhibited abdominal pain, unintentional weight loss, accompanied by nausea and vomiting— a constellation of symptoms that poses a significant diagnostic challenge, given their overlap in both malignancy and SMA syndrome. Our patient’s significant weight loss prior to presentation likely exacerbated the anatomical narrowing responsible for SMA syndrome. Furthermore, tumor-related cachexia likely resulted in a reduction of the mesenteric fat pad, further predisposing the patient to SMA syndrome. Given the aggressive nature of SRCC, systemic chemotherapy remains the mainstay of treatment, often utilizing regimens such as FOLFOX or FOLFIRI (5-fluorouracil, leucovorin, and irinotecan), although outcomes remain poor. In our case, managing the underlying cause of SMA syndrome involved tumor reduction through chemotherapy, with the potential for future surgical intervention.
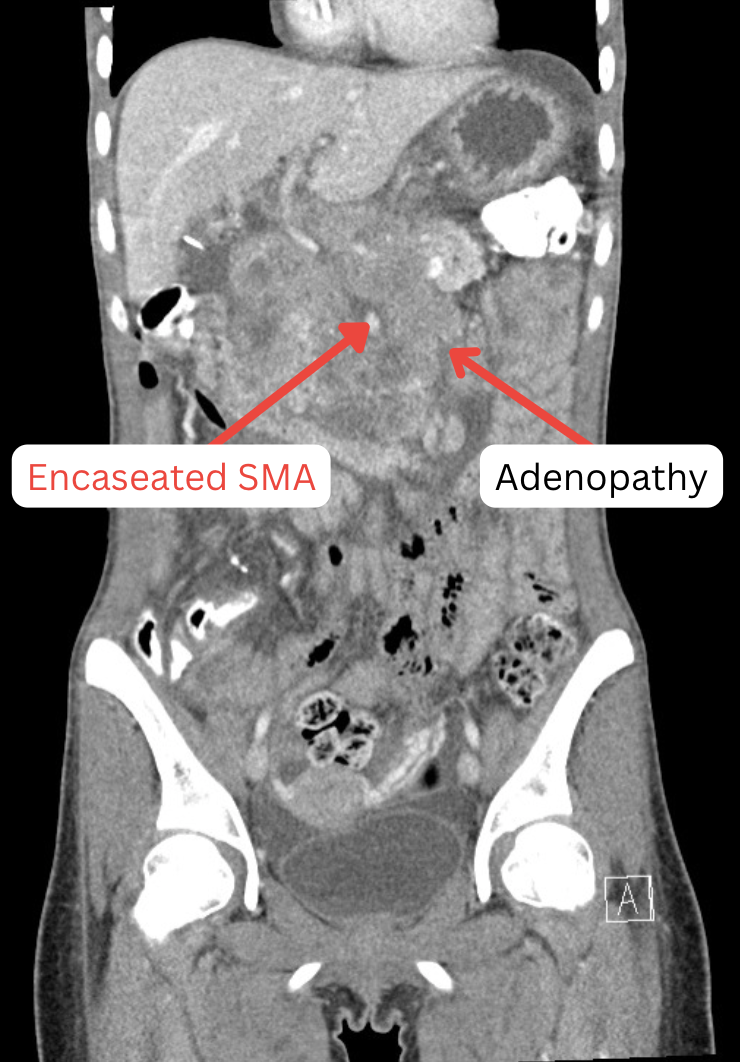
Figure: Figure 1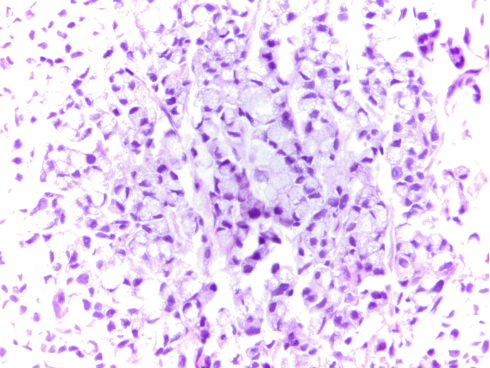
Figure: Figure 2
Disclosures:
Lorraine Chong Tai indicated no relevant financial relationships.
Amanda Eukovich indicated no relevant financial relationships.
Lorraine Chong Tai, MD, Amanda Eukovich, DO. P0371 - A Rare Intersection: A Case of Signet Ring Cell Carcinoma of the Colon Causing SMA Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.