GMERS Medical College and Hospital, Sola Ahmedabad, Gujarat, India
Krupa N. Patel, MBBS1, Manav G. Limbachiya, MBBS2, Nishant Soni, MBBS1, Harsh Patel, MD3, Vivek P. Joshi, DM4 1GMERS Medical College and Hospital, Sola, Ahmedabad, Gujarat, India; 2C U Shah Medical College and hospital, Vadodara, Gujarat, India; 3GMERS Medical College and hospital, Sola, Ahmedabad, Gujarat, India; 4Ansh Hospital, Ahmedabad, Gujarat, India Introduction: Hemophagocytic lymphohistiocytosis (HLH) incidence is < 4 in a million population. Infective etiology accounts for 24.3% of cases and 21.4% mortality. Manifestation of Rectal Strictures observed in this patient is not associated with Inflammatory Bowel Disease (IBD) and is due to HLH which was an atypical finding in our case.
Case Description/
Methods: A 21-year-old male presented with complaints of fever, anorexia, intermittent constipation, anemia, fatigue, and weight loss in the last 9 months. Laboratory investigations revealed pancytopenia [Hb-2.9 g/dL, WBC-1.71 ×10³/mm³, and platelets-22 ×10³/mm³] and neutrophil counts 599 cells/mm³. Serum Biochemistry shows total bilirubin of 1.50 mg/dL, direct bilirubin of 0.40 mg/dL, LDH of 1870 IU/L, and Ferritin of >1500 ng/mL. Bone Marrow examination showed a reversed Myeloid: erythroid (M:E) ratio (1:1.05), Mild hypocellular marrow showing all 3 lineages peripheral pancytopenia, and Hemophagocytosis was observed. Ebstein Barr Virus (EBV) DNA PCR revealed >10,000 copies/mL. Ultrasonography is suggestive of thickened and inflamed walls of the sigmoid colon and rectum, with a maximum thickness of 6-7mm. The liver appears enlarged (16 cm in oblique craniocaudal extension) and normal in echotexture. The spleen seems to be enlarged. Upper gastrointestinal endoscopy (GI) shows Erosive gastritis in the antrum and its histopath reveals chronic active proctitis. A colonoscopy shows fibrotic strictures in the rectum at 10 cm from the anal verge. The scope could not be negotiated beyond and a guidewire was passed, dilation 5,7,9 mm done. Structures extend from 10cm-13cm from the anal verge. Rectal and sigmoid colon shows multiple aphthous ulcers and inflamed mucosa. Rectum histo-path reveals fibrinous material with very few colonic mucosal fragments. Discussion: Initially, the patient was misdiagnosed with IBD and was started on Tab mesalamine but no improvements were noted. GI Histopathology shows no malignancy, IBD, and other inflammatory disorders. Then Secondary HLH due to EBV was diagnosed with HLH criteria. Features of HLH-associated GI complications such as erosive gastritis, and aphthous ulcers seen. This patient had recurrent rectal strictures which required frequent endoscopic balloon dilatation which relieved pain and obstipation. The patient was managed on mesalazine suppository, steroid, tranexamic acid, lidocaine-diltiazem cream, and rituximab. This case emphasizes the diagnostic complexity and highlights the importance of GI symptoms in HLH.
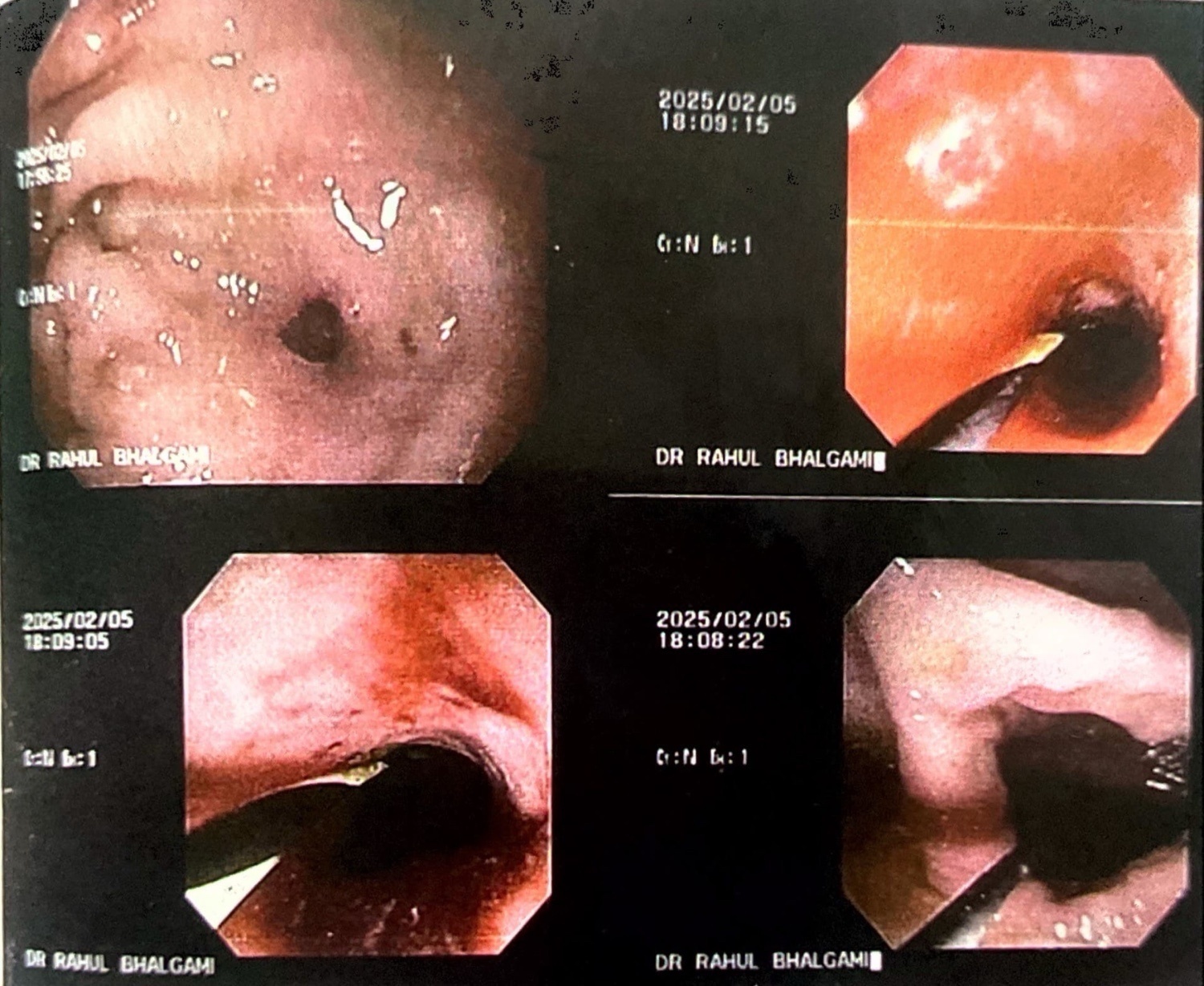
Figure: Colonoscopy reveals proliferative strictures with compromised lumen.
Figure: Colonoscopy shows Fibrotic stricture seen in rectum at 10 cms from anal verge. Rectum and distal sigmoid colon shows multiple aphthous ulcers and inflamed mucosa.
Disclosures: Krupa Patel indicated no relevant financial relationships. Manav Limbachiya indicated no relevant financial relationships. Nishant Soni indicated no relevant financial relationships. Harsh Patel indicated no relevant financial relationships. Vivek Joshi indicated no relevant financial relationships.
Krupa N. Patel, MBBS1, Manav G. Limbachiya, MBBS2, Nishant Soni, MBBS1, Harsh Patel, MD3, Vivek P. Joshi, DM4. P0365 - Recurrent Rectal Strictures in EBV-Associated HLH: A Rare Gastrointestinal Manifestation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")