Charitha Karanam Ramapathy, MD1, Tyler Daugherty, MD2, Dalia Eltoum, MD2, Patricia Ajayi-Fox, MD2 1UAB Montgomery, Montgomery, AL; 2University of Alabama at Birmingham, Birmingham, AL Introduction: Sarcoidosis is a chronic inflammatory disease of unclear origin that can impact multiple organ systems, though it seldom involves the gastrointestinal tract—occurring in fewer than 1% of patients. Colonic involvement is particularly uncommon and typically exhibits vague gastrointestinal symptoms, including abdominal discomfort, diarrhea, unintentional weight loss, and iron deficiency anemia or even bowel obstruction.
Case Description/
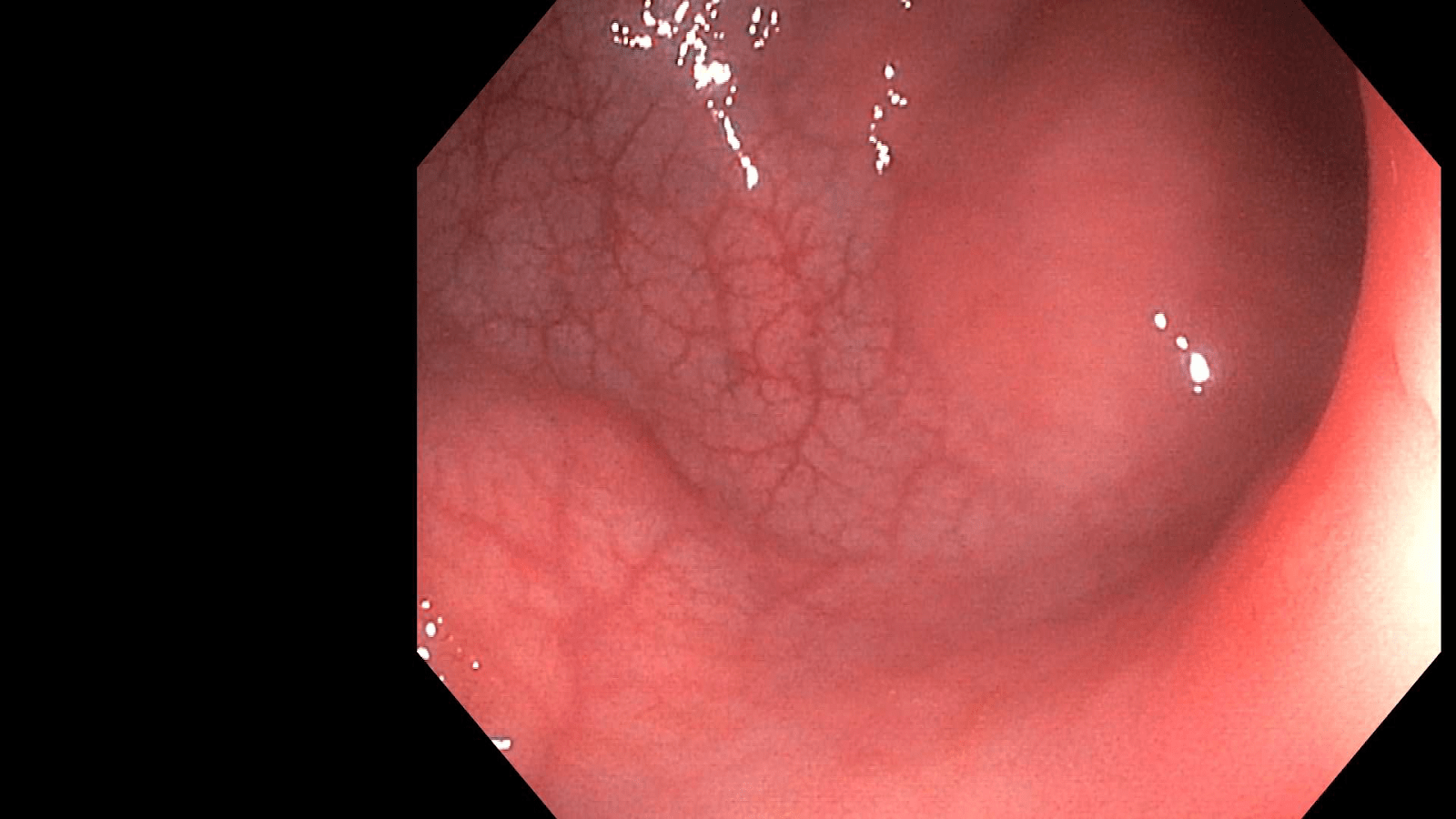
Methods: Patient is a 31-year-old female with no known medical conditions presented with upper abdominal pain for the past 1 year, waxes and wanes, not associated with food intake, has constipation with bowel movement every 4-5 days. She had multiple visits to ED with no definitive diagnosis. AST is 71 units/L, Alkaline phosphatase is 360 units/L. MRCP showed no pancreatic cystic lesions, findings consistent with periportal, mesenteric, retroperitoneal lymphadenopathy measuring about 3.9 x 2. 6cm and right hilar lymphadenopathy as well. She underwent endoscopy and colonoscopy to rule out inflammatory bowel disease. Colonoscopy showed polypoid lesions in the rectum (Figure 1), descending colon, ascending colon and cecum with pathology showing non caseating granulomas and diagnosis of colonic sarcoidosis is confirmed. Angiotensin converting enzyme levels are elevated at 260, quantiferon gold test is negative. She underwent EUS with biopsy of a perigastric lymph node which showed non caseating granulomatous inflammation (Figure 2). Patient is started on prednisone, methotrexate along with bactrim and folic acid. Discussion: Sarcoidosis tends to occur in young and middle aged patients commonly in women. Sarcoidosis and inflammatory bowel disease can present with overlapping extraintestinal symptoms such as joint inflammation, skin conditions like erythema nodosum, and eye involvement including uveitis. Other potential differential diagnoses include granulomatous inflammation due to hypersensitivity reactions, tuberculosis, syphilis, fungal diseases and cancer. Diagnosing colonic sarcoidosis is difficult and the defining feature of sarcoidosis in biopsy samples is the presence of noncaseating granulomas. Treatment is generally not indicated for asymptomatic patients. Corticosteroids are typically effective and are preferred treatment for those with symptomatic disease. Gastrointestin al sarcoidosis is a diverse and potentially serious condition that demands early recognition and a collaborative, multidisciplinary strategy to ensure tailored treatment and ongoing care.
Figure: Figure 1
Figure: Figure 2
Disclosures: Charitha Karanam Ramapathy indicated no relevant financial relationships. Tyler Daugherty indicated no relevant financial relationships. Dalia Eltoum indicated no relevant financial relationships. Patricia Ajayi-Fox indicated no relevant financial relationships.
Charitha Karanam Ramapathy, MD1, Tyler Daugherty, MD2, Dalia Eltoum, MD2, Patricia Ajayi-Fox, MD2. P0455 - Colonic Sarcoidosis: A Rare Culprit Behind Chronic Abdominal Pain, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")