Sunday Poster Session
Category: Colon

Frank Lin, DO
St. Luke's University Health Network
Bethlehem, PA
A 49-year-old male initially presented for nausea, vomiting, epigastric abdominal pain, and diarrhea with hematochezia. Prior to presentation, the patient had been taking amoxicillin for four days for antibiotic prophylaxis after a dental extraction. Stool studies and infectious work-up were unremarkable.
After his first episode of colitis with suspicion for possible infectious etiology, the patient was placed on amoxicillin-clavulanate despite unremarkable infectious work-up. He was subsequently re-admitted to the hospital with recurrent symptoms of hematochezia, diarrhea, abdominal pain, and vomiting. Clostridium difficile testing was negative during the second admission. An ultrasound of the celiac and mesenteric vessels showed patency of the celiac, super mesenteric, inferior mesenteric, splenic, and common hepatic arteries. CT angiography of the abdomen and pelvis showed acute severe colitis with involvement of the rectosigmoid colon, which was spared on CT angiography during the initial admission.
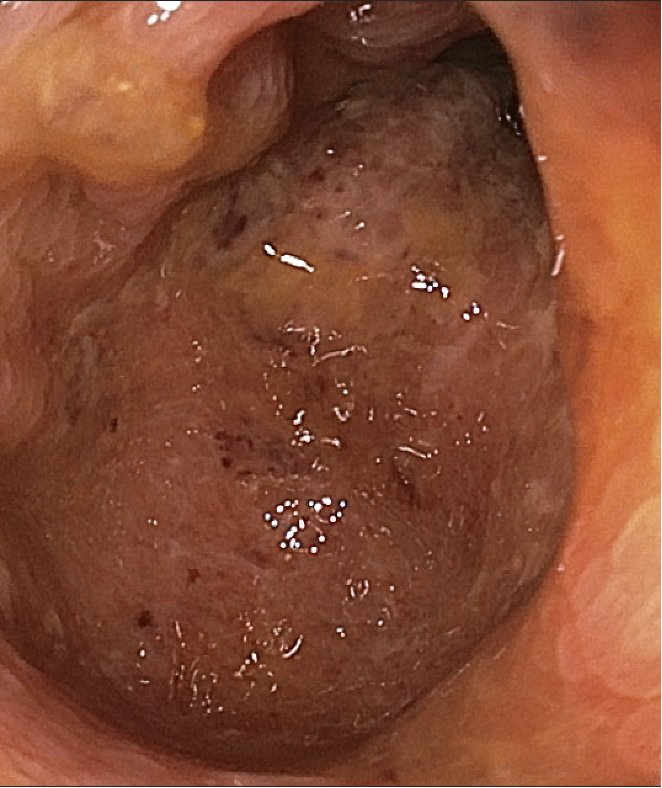
Colonoscopy showed severe edematous and ulcerated mucosa with loss of vascular pattern in the hepatic flexure consistent with ischemic colitis (Figure 1). Biopsy of the colonic mucosa at the hepatic flexure was compatible with ischemic-type mucosal injury and colitis without evidence for dysplasia or malignancy (Figures 2). Autoimmune work-up was entirely unremarkable, hence there was low concern for vasculitis. A three-month follow-up colonoscopy showed complete resolution of ischemic colitis.