Colin Hartgerink, MD1, Joan W. Chen, MD, MS2 1University of Michigan, Ann Arbor, MI; 2University of Michigan Health, Ann Arbor, MI Introduction: Herpes simplex virus (HSV) rarely causes esophagitis in immunocompetent patients. Here, we present a case of HSV esophagitis in an otherwise healthy 24-year-old male.
Case Description/
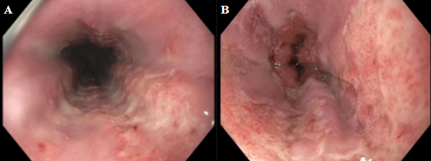
Methods: A 24-year-old male with a past medical history of gastroesophageal reflux disease (GERD) presented with a one-week history of nausea, vomiting, odynophagia, epigastric pain, fevers, and a sore throat. He reported significant odynophagia and epigastric abdominal pain with any oral intake including liquids. Upper endoscopy a year prior had shown gastritis for which patient had been taking pantoprazole 20 mg twice daily and famotidine 40 mg daily. Physical exam showed bilateral tonsillar hypertrophy without purulence or erythema. Labs were notable for negative Strep A polymerase chain reaction (PCR), negative mononucleosis screen, negative CMV IgM, Westergren RBC sedimentation rate elevated to 61, and negative Helicobacter pylori stool antigen. Subsequent esophagogastroduodenoscopy 4 days after initial presentation revealed severe esophagitis with only small patchy areas of mucosal sparing (Figure 1A and 1B). Esophageal biopsy was consistent with herpes esophagitis with positive staining for HSV 1/2. He did report a history of cold sores but denied any recent cold sores. He was treated with acyclovir 400 mg three times daily for 7 days. A repeat EGD was recommended in 6-12 months to assess for underlying eosinophilic esophagitis but was never completed as the patient was lost to follow up. Discussion: Although much more commonly seen in immunocompromised patients, herpes esophagitis has been reported in immunocompetent hosts. Literature on herpes esophagitis in immunocompetent individuals is limited however the disease mainly affects young males without other significant comorbidities. The mechanism is not fully understood, however disruption of esophageal mucosal such as secondary to gastroesophageal reflux, eosinophilic esophagitis, or esophageal instrumentation is thought to increase the risk of herpes esophagitis. The disease is usually self-limited, but acyclovir therapy may hasten resolution of symptoms. Although rare, herpes esophagitis should be on the differential for immunocompetent patients presenting with odynophagia, fevers, and retrosternal or epigastric pain.
Figure: Figure 1A: Middle third of esophagus; Figure 1B: Lower third of esophagus
Disclosures: Colin Hartgerink indicated no relevant financial relationships. Joan Chen: Phathom Pharmaceuticals – Consultant.
Colin Hartgerink, MD1, Joan W. Chen, MD, MS2. P0776 - A Rare Case of Herpes Simplex Virus Esophagitis in an Immunocompetent Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.