Owen Battel, MD1, Gianna Stoleru, MD1, Rebecca Haug, MD2 1University of Virginia, Charlottesville, VA; 2University of Virginia Medical Center, Charlottesville, VA Introduction: Duodenal perforations are commonly caused by peptic ulcer disease, iatrogenic injury, or trauma; they are rarely seen as a complication of nasogastric (NG) tube placement. Gastric decompression and antibiotics for small perforations or surgical repair for larger or unstable perforations have been the standard of care for treatment. However, recent literature has highlighted endoscopic management as a safe and effective alternative, recommending this be attempted for all acute iatrogenic perforations related to advanced endoscopic therapies. Repairs have been successful using endoclips, over-the-scope clips, and endoscopic suturing. Despite expanding literature, there remains no consensus of whether to pursue conservative, surgical, or endoscopic management in the setting of iatrogenic perforations. We present a rare case of duodenal perforation from NG tube placement successfully controlled with OVESCO over-the-scope clip placement.
Case Description/
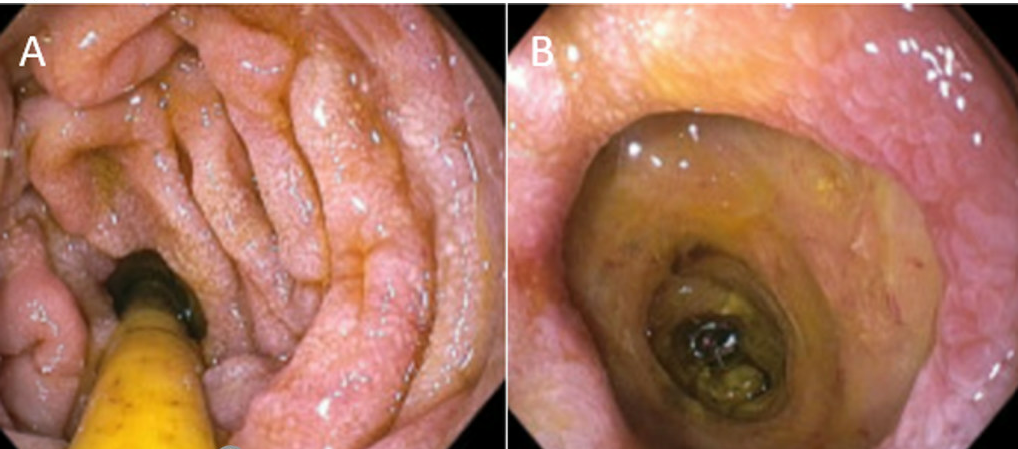
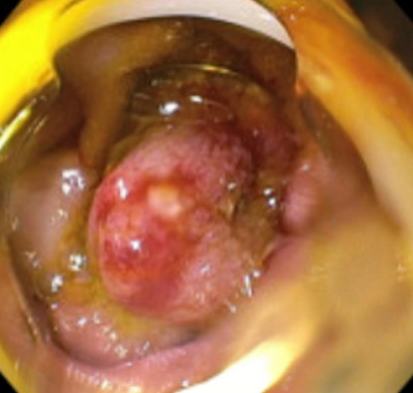
Methods: A 78-year-old female was transferred to University of Virginia for further evaluation of progressive neuromuscular weakness and dysphagia. Prior to transfer, she underwent NG tube placement for enteral feeding after multiple failed swallow evaluations. The patient was later found to have anemia and melanic stool, for which she was treated medically with proton pump inhibitors prior to undergoing endoscopic evaluation for anemia. During upper endoscopy, her NG tube was found to be distally located in a false lumen past the second portion of the duodenum, consistent with retroperitoneal perforation. There was ulceration and inflammation of the surrounding mucosa without active bleeding. The NG tube was removed and an OVESCO clip was deployed to close the defect. Post-procedural imaging supported successful closure of the defect, and the patient’s GI bleeding resolved. NG tube was replaced in the stomach, but patient ultimately expired due to neuromuscular disease. Discussion: Endoscopic repair of duodenal perforations is an emerging practice; however, there is a scarcity of research surrounding this topic in the setting of iatrogenic perforations. The development of a duodenal perforation from NG tube placement is unique and posed a challenging clinical scenario, given the chronicity of the iatrogenic perforation was unclear and she was not considered to be a surgical candidate given her frailty and underlying neuromuscular disease. Ultimately endoscopic intervention with OVESCO clip for closure of the iatrogenic perforation was successful.
Figure: Figure 1: False lumen distal to enteral feeding tube
Figure: Figure 2: OVESCO deployed to close false lumen
Disclosures: Owen Battel indicated no relevant financial relationships. Gianna Stoleru indicated no relevant financial relationships. Rebecca Haug indicated no relevant financial relationships.
Owen Battel, MD1, Gianna Stoleru, MD1, Rebecca Haug, MD2. P0900 - Use of OVESCO Clip for Closure of Duodenal Perforation Caused by Enteral Feeding Tube Placement, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.