Cooper Medical School of Rowan University Camden, NJ
Shrey Dalwadi, BS1, Zehara Abidi, MS2, Avneet Singh, DO3, Fariha Hasan, MD3, Alexander Garcia, DO3 1Cooper Medical School of Rowan University, Camden, NJ; 2Touro College of Osteopathic Medicine, Harlem, NY; 3Cooper University Health Care, Camden, NJ Introduction: Upper gastrointestinal bleeding (GIB) originates above the ligament of Treitz and is commonly caused by ulcerative and erosive lesions or less commonly due to vascular lesions or masses. While most upper GIBs can be identified via endoscopy, the source of bleeding remains unidentified in 10–15% of cases. A Dieulafoy lesion (DL) is a vascular malformation of the gastrointestinal tract that accounts for 1-2% of all GIB. DLs are typically asymptomatic, but can cause intermittent bleeding or massive hemorrhage. This case presents a 25-year-old female with unstable hemoglobin levels following a cesarean section (CS) delivery, subsequently found to be massive blood loss secondary to DL.
Case Description/
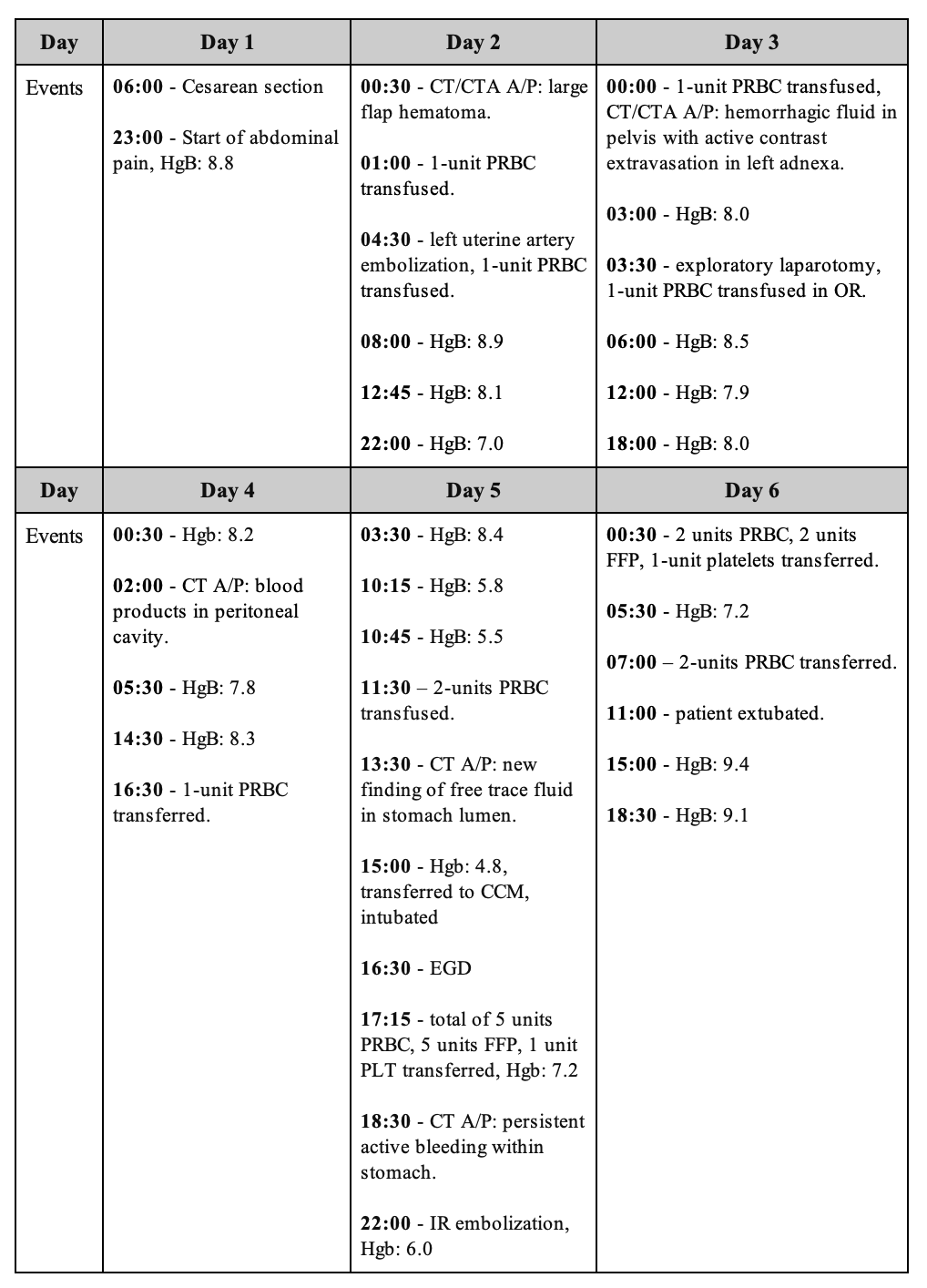
Methods: A 25-year-old female with a history of GERD and prior CS presented to obstetric triage at 35 weeks gestation with contractions. The evening following expedited CS, she developed acute onset abdominal pain and was found to have reduced hemoglobin levels (8.8 g/dL compared to 9.9 g/dL at admission). CTA showed hemo-pneumoperitoneum secondary to a left uterine artery bleed that required laparoscopic intervention with successful ligation. The following day (Table 1), she was noted to have a 3 g/dL drop in hemoglobin. Repeat CTA showed new free fluid in the stomach lumen. An urgent bedside esophagogastroduodenoscopy demonstrated a bleeding DL (Figure 1). There was stigmata of recent bleeding on the lesser curvature of the stomach and a few non-bleeding duodenal ulcers without stigmata of bleeding. Temporary hemostasis was achieved using two hemostasis clips and EndoClot® Submucosal Injection Solution with complete hemostasis using coil embolization. The patient was discharged after hemoglobin stabilization. Discussion: DL is an infrequent, but potentially life threatening source of upper GIB. There is continuous debate regarding the origin of DL bleeding. Studies have suggested a link between DL bleeds and chronic utilization of anticoagulants and nonsteroidal anti-inflammatory drugs. Given the rarity of DL in a patient of this age, it must be considered if physiologic adaptations such as expanded blood volume and hormonal shifts in gestation may serve as triggers. In addition to endoscopic clipping, coil embolization may be recommended for refractory bleeding. Overall, this report underscores the need to consider this rare, yet dangerous cause of GIB in obstetrics patients.
Figure: Table 1: Timeline of hemoglobin levels (in units of g/dL) and pertinent interventions that occurred on days 1-6
Figure: Figure 1. A-C. Esophagogastroduodenoscopy of a Dieulafoy lesion (A, B) on the lesser curvature of the stomach (C) causing oozing bleeding denoted by yellow arrows.
Disclosures: Shrey Dalwadi indicated no relevant financial relationships. Zehara Abidi indicated no relevant financial relationships. Avneet Singh indicated no relevant financial relationships. Fariha Hasan indicated no relevant financial relationships. Alexander Garcia indicated no relevant financial relationships.
Shrey Dalwadi, BS1, Zehara Abidi, MS2, Avneet Singh, DO3, Fariha Hasan, MD3, Alexander Garcia, DO3. P0980 - Dieulafoy Lesion: A Rare Cause of Postpartum Bleeding, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.