P1047 - Pattern of Joint Distribution in Peripheral Arthritis Does Not Alter Health-Related Quality of Life Across Multiple Patient-Reported Outcomes – Results From the CHASE Cohort
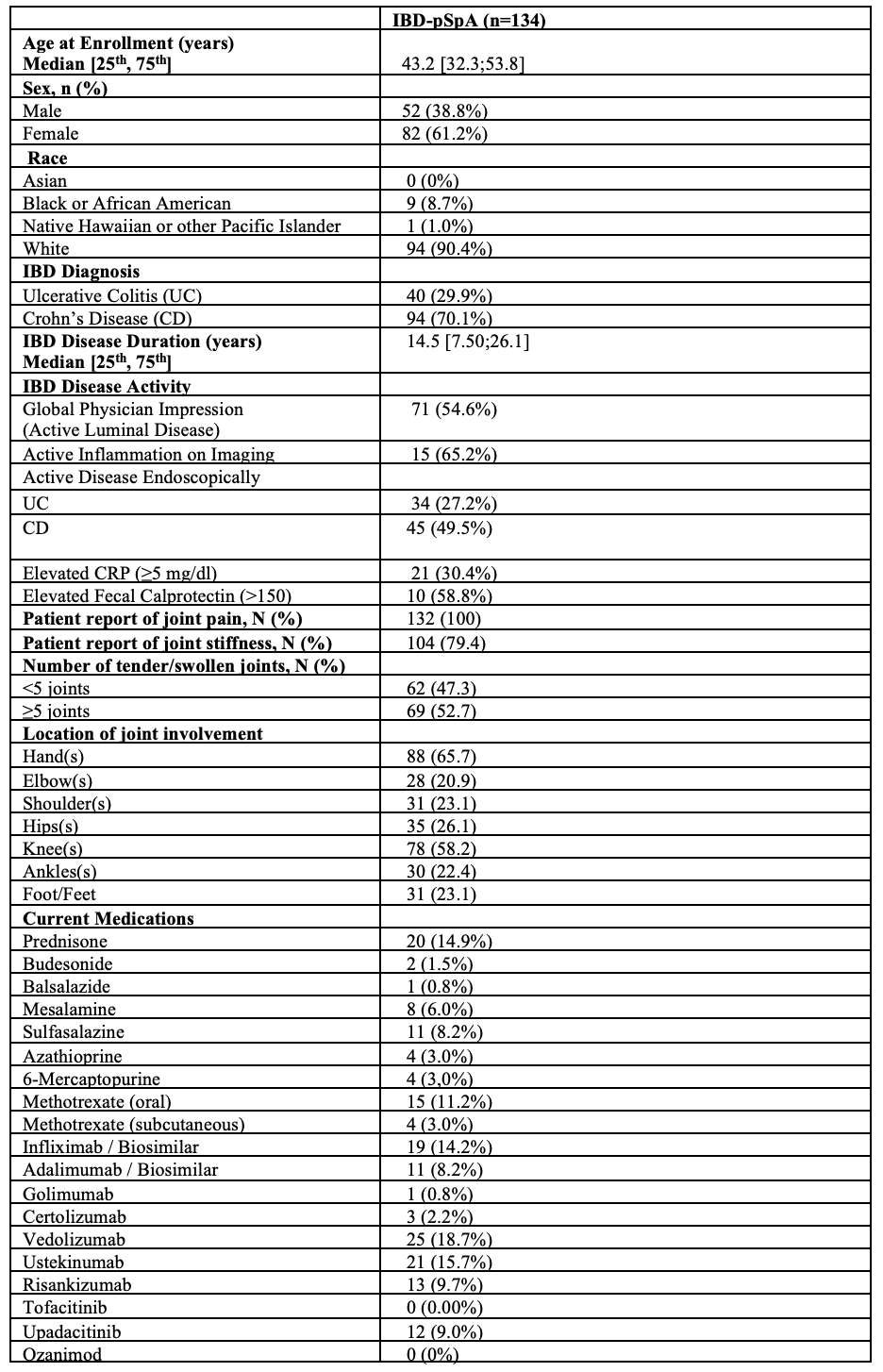
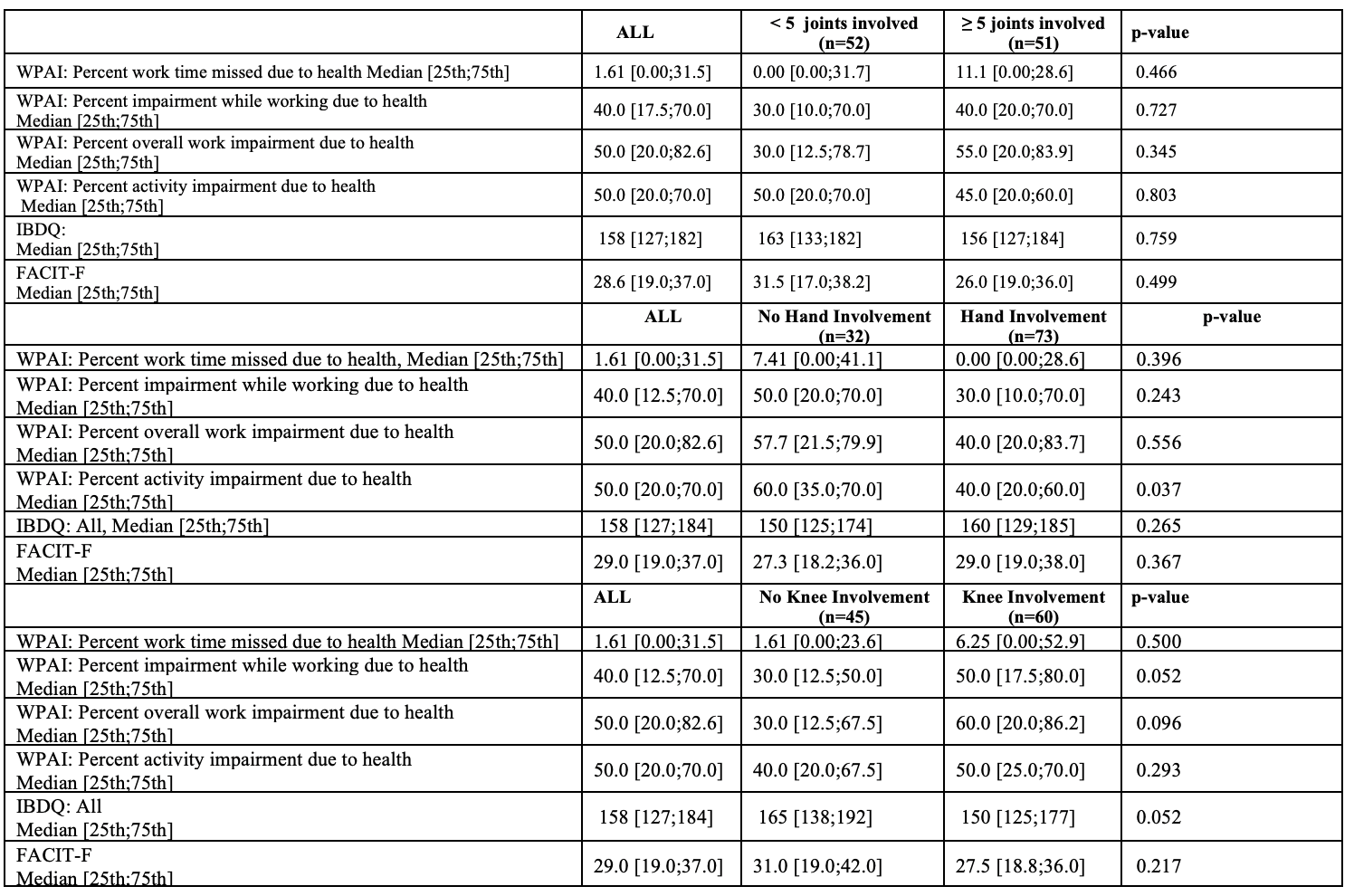
Katherine Falloon, MD1, Suha Abushamma, MD1, Ashwin Ananthakrishnan, 2, Edward L. Barnes, MD, MPH3, Abhik Bhattacharya, MD4, Raymond K. Cross, MD, MS, FACG5, Shashank Cheemalavagu, MD1, Jean-Frederic Colombel, MD4, Emily Gore, MD4, Hans Herfarth, MD, PhD6, Sara Horst, MD, MPH, FACG7, M. Elaine Husni, MD1, Jeremy A.. Klein, MD8, Dana J. Lukin, MD, PhD, FACG9, David T. Rubin, MD10, Ellen J. Scherl, MD9, Taha Qazi, MD1, Qijun Yang, MS11, Benjamin L. Cohen, MD1, Brian G. Feagan, MD12, Florian Rieder, MD1 1Cleveland Clinic Foundation, Cleveland, OH; 2Division of Gastroenterology, Massachusetts General Hospital and Harvard Medical School, Boston, MA; 3Multidisciplinary Inflammatory Bowel Diseases Center, Division of Gastroenterology and Hepatology, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA, Chapel Hill, NC; 4Icahn School of Medicine at Mount Sinai, New York, NY; 5The Melissa L. Posner Institute for Digestive Health & Liver Disease, Mercy Medical Center, Baltimore, MD; 6University of North Carolina at Chapel Hill, Chapel Hill, NC, USA, Chapel Hill, NC; 7Vanderbilt University School of Medicine, Nashville, TN; 8University of Chicago Medicine, Inflammatory Bowel Disease Center, Chicago, IL; 9Jill Roberts Center for Inflammatory Bowel Disease, Weill Cornell Medicine, New York, NY; 10University of Chicago Medicine Inflammatory Bowel Disease Center, Chicago, IL, USA, Chicago, IL; 11Cleveland Clinic, Cleveland, OH; 12Division of Gastroenterology, Department of Medicine, University of Western Ontario and Alimentiv, London, ON, Canada Introduction: Inflammatory bowel disease (IBD)-associated peripheral spondylarthritis (IBD-pSpA) is common but not well studied, with limited research regarding impact on health-related quality of life (HRQoL). The type I vs type II classification schema, which groups patient based on the distribution, number and size of involved joints, is commonly utilized in the gastroenterology literature. However, this schema is neither widely accepted within the rheumatology literature nor prospectively validated. The aim of this study was to evaluate whether the HRQoL scores vary based on the type I vs type II classification schema. Methods: We prospectively recruited patients with IBD-pSpA, defined by previously established consensus criteria via the Cohort for Healing Arthritis, Skin, and Eye Extra-Intestinal Manifestations (CHASE-EIM) from six sites across the United States. The relationship of clinical presentation of IBD-pSpA (number and type of involved peripheral joints) on HRQoL was assessed via three previously validated patient reported outcomes – the Inflammatory Bowel Disease Questionnaire (IBDQ), the Work Productivity and Activity Impairment Questionnaire (WPAI), and the Functional Assessment of Chronic Illness Therapy – Fatigue (FACIT-F). Analyses were performed using R software and a significance level of 0.05 was assumed for all tests. Results: 134 patients with IBD-pSpA (61.2% female, 70.1% with CD) were included in the analysis (Table 1). 47.3% of patients had < 5 joints involved and the remainder ≥5. Hands (65.7%) and knees (58.2%) were the most commonly involved joints. 103 patients completed the requested questionnaires (76.9%). There were no statistically significant differences in any of the questionnaire scores based on number of swollen or tender joints or location of swollen or tender joints (Table 2, data for hands and knees reported; data for other joints not shown but no statistically significant differences identified). Discussion: Pattern of joint involvement did not influence HRQoL across multiple previously validated PROs (IBDQ, WPAI, and FACIT-F) in patients with IBD-pSpA, casting additional doubt regarding the clinical utility of the type I vs type II classification schema in this patient population. Development of a novel PRO specific to IBD-pSpA will provide further insights into the clinical impact of IBD-pSpA and is currently underway by our group.
Figure: Table 1: Baseline Demographics and Clinical Characteristics IBD-pSpA = inflammatory bowel disease associated peripheral spondyloarthritis, CRP = C reactive protein
Figure: Table 2: Questionnaire Scores Based on Pattern of Joint Involvement
WPAI = work productivity and activity impairment questionnaire, IBDQ = inflammatory bowel disease questionnaire, FACIT=F = functional assessment of chronic illness therapy
Katherine Falloon, MD1, Suha Abushamma, MD1, Ashwin Ananthakrishnan, 2, Edward L. Barnes, MD, MPH3, Abhik Bhattacharya, MD4, Raymond K. Cross, MD, MS, FACG5, Shashank Cheemalavagu, MD1, Jean-Frederic Colombel, MD4, Emily Gore, MD4, Hans Herfarth, MD, PhD6, Sara Horst, MD, MPH, FACG7, M. Elaine Husni, MD1, Jeremy A.. Klein, MD8, Dana J. Lukin, MD, PhD, FACG9, David T. Rubin, MD10, Ellen J. Scherl, MD9, Taha Qazi, MD1, Qijun Yang, MS11, Benjamin L. Cohen, MD1, Brian G. Feagan, MD12, Florian Rieder, MD1. P1047 - Pattern of Joint Distribution in Peripheral Arthritis Does Not Alter Health-Related Quality of Life Across Multiple Patient-Reported Outcomes – Results From the CHASE Cohort, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.