Katherine L.. Stone, MD1, Ellen M. Axenfeld, MD2, Lisa Malter, MD, FACG3 1NYU Langone Health, New York, NY; 2NYU Langone Health Inflammatory Bowel Disease Center, New York, NY; 3Division of Gastroenterology, Department of Medicine, NYU Langone Health, New York, NY Introduction: Crohn’s disease (CD) is a chronic immune-mediated inflammatory disease that can affect any site of the gastrointestinal tract, including rare oropharyngeal involvement. Diagnosing oropharyngeal CD can be difficult due to its nonspecific symptoms and broad differential. We present, to our knowledge, the first case of an oropharyngeal mass ultimately confirmed as oropharyngeal CD that was non-responsive to anti-TNF therapy with robust response to upadacitinib.
Case Description/
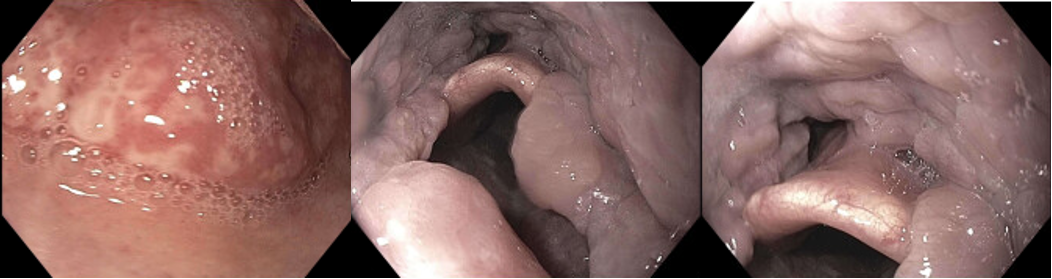
Methods: A 74-year-old male with a 7-year history of colonic and perianal CD on infliximab presented to the emergency room in April 2021 with pharyngitis. CT neck showed tonsillar enlargement, soft palate edema, and a mass-like oropharyngeal structure. Antibiotics provided no relief. Biopsy via laryngoscopy ruled out malignancy and revealed non-necrotizing granulomas. Upper endoscopy showed nodular mucosa in the posterior oropharynx (Figure 1). Symptoms persisted despite high-dose oral steroids. Workup for sarcoidosis and vasculitis was negative. Due to atypical findings, diagnosis remained uncertain. After multidisciplinary review, oropharyngeal CD was deemed the most likely etiology. Of note, infliximab drug level remained elevated ( >30) throughout this course without anti-drug antibodies and without alternative evidence of active luminal or perianal CD.
In June 2024, the patient was hospitalized with 50 lb weight loss and severe dysphagia. IV steroids were started, and a percutaneous gastrostomy tube was placed. Infliximab was discontinued, and upadacitinib 45mg induction began. Over several weeks, oropharyngeal pain improved. By September 2024, he tolerated a full diet and passed a barium swallow. December laryngoscopy showed resolution of lymphoid proliferation, and repeat endoscopy was unremarkable (Figure 2). His gastrostomy tube was removed. After 12 weeks of induction, he transitioned to upadacitinib 30mg maintenance without recurrence. Discussion: This appears to be the first documented case of mass-like oropharyngeal CD responsive to upadacitinib. Diagnosis and escalation were delayed by atypical presentation, lack of classic CD mucosal features, and non-response to anti-TNF therapy. Ultimately, the histopathologic presence of non-necrotizing granulomatous inflammation and response to upadacitinib support the diagnosis. This case underscores the importance of considering atypical CD manifestations and the value of multidisciplinary collaboration in managing complex disease.
Figure: Figure 1: Initial upper endoscopy showing nodular mucosa in the posterior oropharynx
Figure: Figure 2: Repeat upper endoscopy showing resolution of lymphoid proliferation after initiating upadacitinib
Disclosures: Katherine Stone indicated no relevant financial relationships. Ellen Axenfeld indicated no relevant financial relationships. Lisa Malter: AbbVie – Grant/Research Support. Bristol Myers Squibb – Advisory Committee/Board Member. Celltrion – Advisory Committee/Board Member. Janssen – Grant/Research Support. Pfizer – Advisory Committee/Board Member, Consultant, Grant/Research Support. Pharmacosmos – Consultant.
Katherine L.. Stone, MD1, Ellen M. Axenfeld, MD2, Lisa Malter, MD, FACG3. P1251 - Mass-Like Oropharyngeal Crohn’s Disease Responsive to Upadacitinib, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.