Ochsner University Hospital & Clinics Lafayette, LA
Samar Mahmood, MD, Amit Rajkarnikar, MD, Melanie Bienvenu, MD, MPH, Christopher Wexler, MD Ochsner University Hospital & Clinics, Lafayette, LA Introduction: HIV disease related Kaposi's sarcoma (KS) is the most common neoplasm caused by human herpesvirus-8. Skin involvement is the most common initial presentation and seen in up to 60% of cases. Visceral involvement is seen with the gastrointestinal (GI) tract and lungs; however, without cutaneous lesions it is rare and fatal if untreated. Most patients with GI involvement are asymptomatic, but may present with non-specific symptoms such as weight loss, vomiting, diarrhea, and abdominal pain.
Case Description/
Methods: 40-year-old male with HIV, chronic Hepatitis B, treated neurosyphilis, and polysubstance use presented to the emergency department with 2–3 months of worsening nausea and vomiting. He reported bilious emesis, poor oral intake, lower abdominal pain, and intermittent productive cough. He had been admitted twice in the last month for similar symptoms. Of note, he started combined antiretroviral therapy (cART) about 3 months prior. HIV viral load was 94 (down from 1.31 million), CD4 count of 74 cells/μL (18 nadir). Chest Xray and KUB were unremarkable. CTA chest revealed patchy right upper lobe consolidation, a distended fluid-filled esophagus, and persistently distended stomach and duodenum. A CT abdomen/pelvis with contrast showed distended stomach and proximal duodenum and enlarged lymph nodes throughout the mesentery. Nasogastric tube was placed for decompression and an EGD was done to evaluate gastric outlet obstruction. EGD showed a 6 mm superficial esophageal ulcer, large gastric nodules with ulcerations, and diffuse inflammation and edema of the second part of the duodenum without ability to transverse the gastroscope beyond. Biopsies taken showed spindle cell vascular proliferation consistent with Kaposi sarcoma, with HHV-8 positivity. He remained NPO with TPN support. Due to high disease burden in the small bowel, he was deemed too high of a risk for surgical intervention by Surgical Oncology. Given his functional and nutritional status, chemotherapy was not an option. He was discharged home with hospice care. Discussion: This case highlights an infrequent presentation of KS-GI. Clinicians should maintain a high degree of suspicion and recommend endoscopic evaluation in advanced HIV disease patients who present with GI symptoms, even if on cART. Screening endoscopy should also be considered for high-risk individuals (low CD4 cell count of < 100 cells/μL, MSM, and presence of cutaneous KS) to allow for appropriate and timely management.
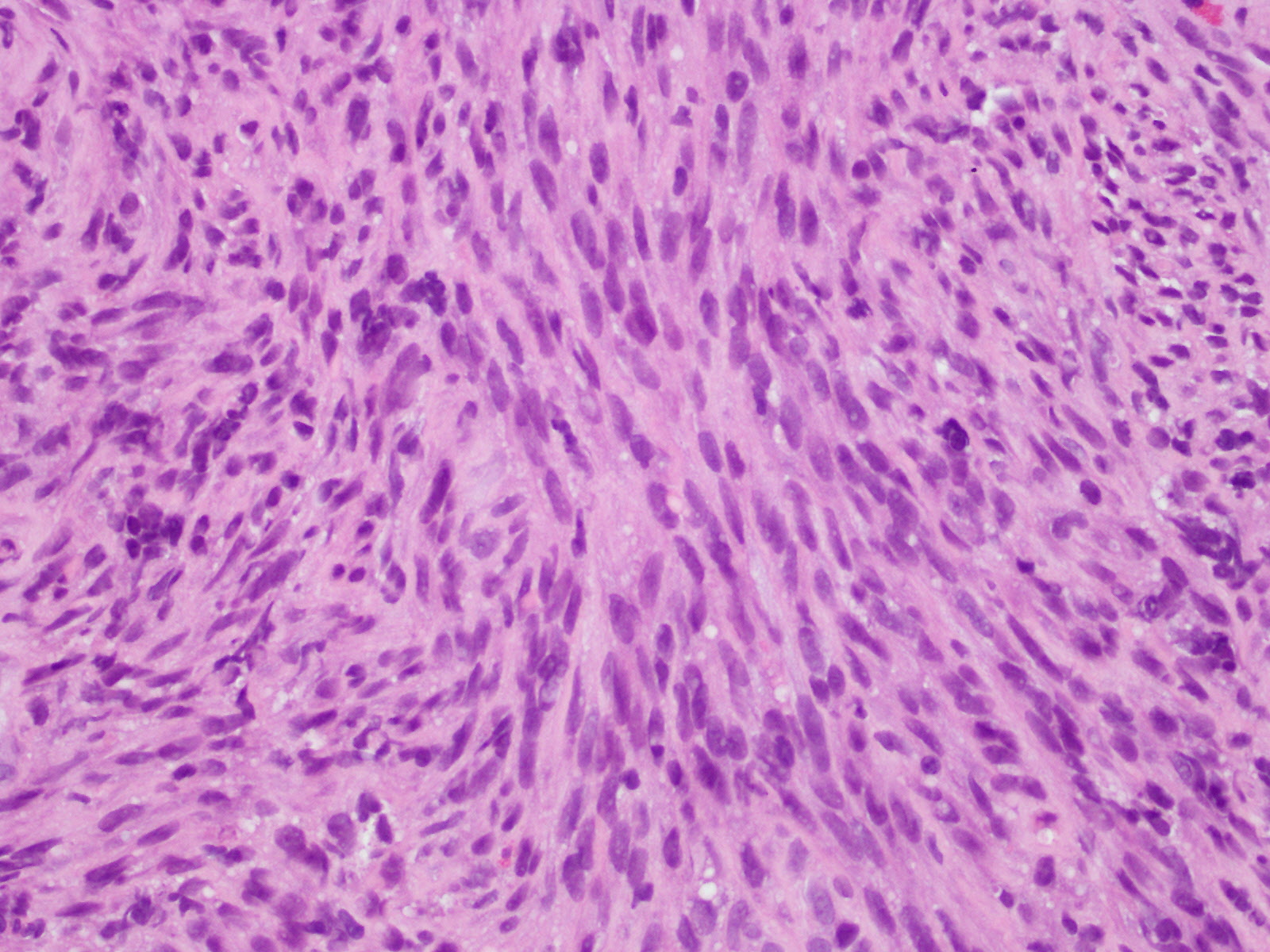
Figure: H&E stain of Duodenal mucosa showing expansion of lamina propria by spindle cell proliferation
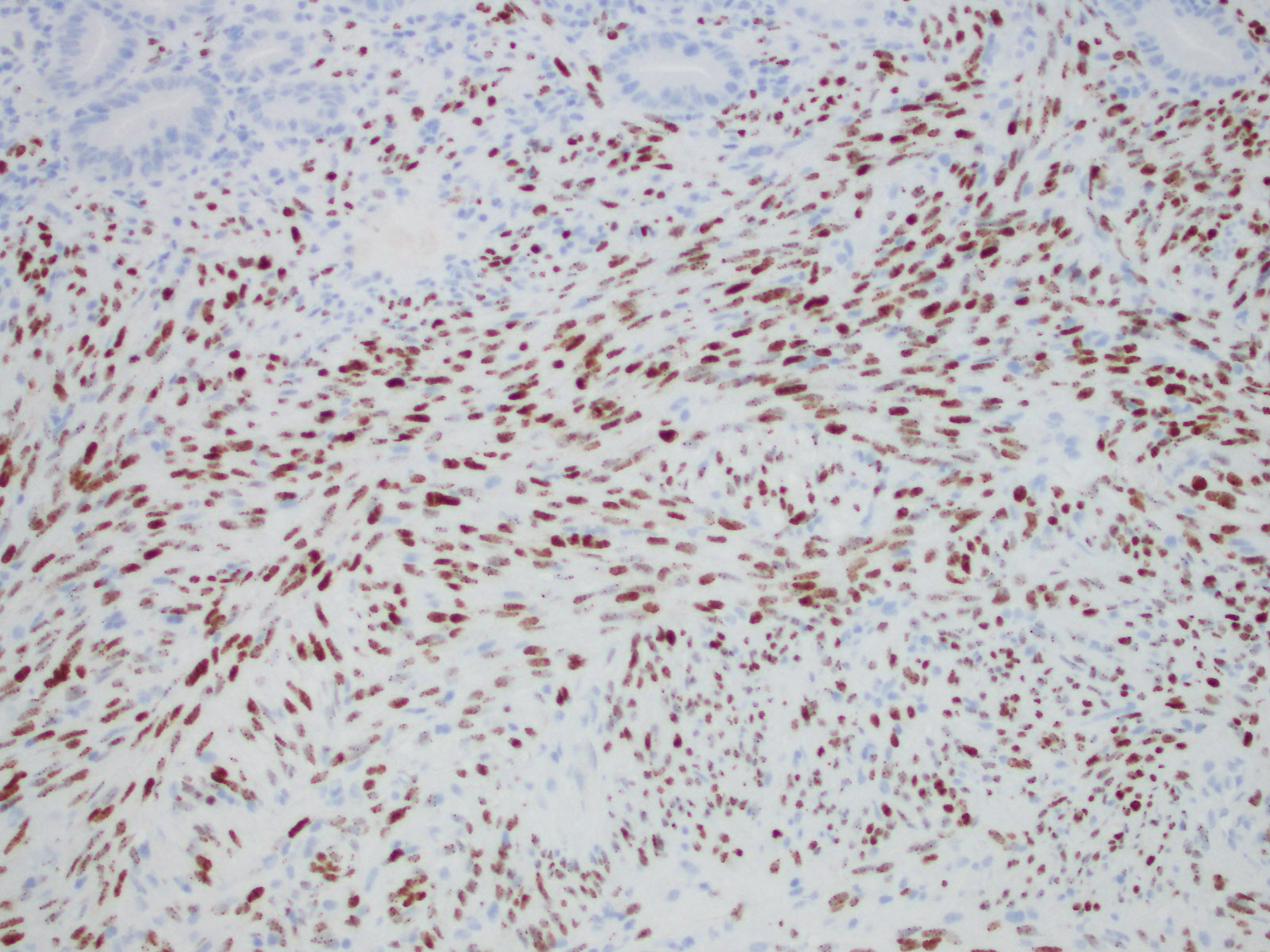
Figure: HHV-8 immunohistochemical stain reveal Kaposi sarcoma cells that show nuclear expression of Human Herpes virus-8
Disclosures: Samar Mahmood indicated no relevant financial relationships. Amit Rajkarnikar indicated no relevant financial relationships. Melanie Bienvenu indicated no relevant financial relationships. Christopher Wexler indicated no relevant financial relationships.
Samar Mahmood, MD, Amit Rajkarnikar, MD, Melanie Bienvenu, MD, MPH, Christopher Wexler, MD. P1313 - Gastric Outlet Obstruction Secondary to Kaposi's Sarcoma: An Uncommon Presentation of a Common Malignancy in Advanced HIV Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")