Ochsner University Hospital & Clinics Lafayette, LA
Amit Rajkarnikar, MD1, Vy Luong, DO1, Alexandra Hebert, MS2, Melanie Bienvenu, MD, MPH1, Shantell Ceaser Ford, MD1, Christopher Wexler, MD1 1Ochsner University Hospital & Clinics, Lafayette, LA; 2LSU Health New Orleans School of Medicine, New Orleans, LA Introduction: Whipple's disease (WD) is a chronic infectious disease caused by a gram-positive bacterium, Tropheryma whippelii, a bacterium found ubiquitously in the environment. WD is an exceedingly rare condition with an overall incidence of about 1-3 in every 1 million people. It is predominant in middle-aged white men. We report a case of an African American male with chronic diarrhea after prolonged and inflammatory arthralgias with histologic evidence confirming Whipple's disease.
Case Description/
Methods: A 58-year-old male with seronegative rheumatoid arthritis was admitted for complaints of abdominal bloating and chronic diarrhea. He reported frequent watery diarrhea of 10 or more episodes and nocturnal awakenings without rectal bleeding or melena over the last 1-2 years with associated weight loss of about 80 lbs. Prior infectious work-up was overall negative. Tissue transglutaminase Ab, IgA/IgG was negative. Multiple CT scan of the abdomen/pelvis resulted in nonspecific findings of enteritis. Patient underwent EGD and colonoscopy where one sessile duodenal polyp was observed. The terminal ileum and entire examined portion of the colon appeared normal. Biopsies later revealed duodenal mucosa with villous blunting and lamina propria expansion by numerous foamy macrophages. Scattered dilated lacteals and fat droplets and abundant positive periodic acid-Schiff (PAS) foamy macrophages were consistent with Whipple’s disease. He underwent lumbar puncture and CSF studies were negative for CNS involvement including negative T. whipplei CSF PCR. The T. whipplei blood PCR was positive. He was treated with IV Ceftriaxone 2 g once daily for 14 days with improvement of his symptoms. He was discharged with Doxycycline 100 mg twice daily and Hydroxychloroquine 200 mg three times daily for maintenance therapy for 12 months. Discussion: WD is a rare, chronic multisystem infection. Pathogenesis interferes with macrophages resulting in dysfunction of host cell degradation. Prodromal stage is characterized by migratory arthralgias involving the large peripheral joints. Systemic phase has symptoms of diarrhea, abdominal pain, weight loss, hepatosplenomegaly, and anemia. Neurologic involvement may occur during or following the systemic presentation. Although a rare condition, Whipple's disease should be suspected with prolonged arthralgias and gastrointestinal involvement. Early recognition of WD is crucial to ensure prompt treatment and proper surveillance and follow-up care.
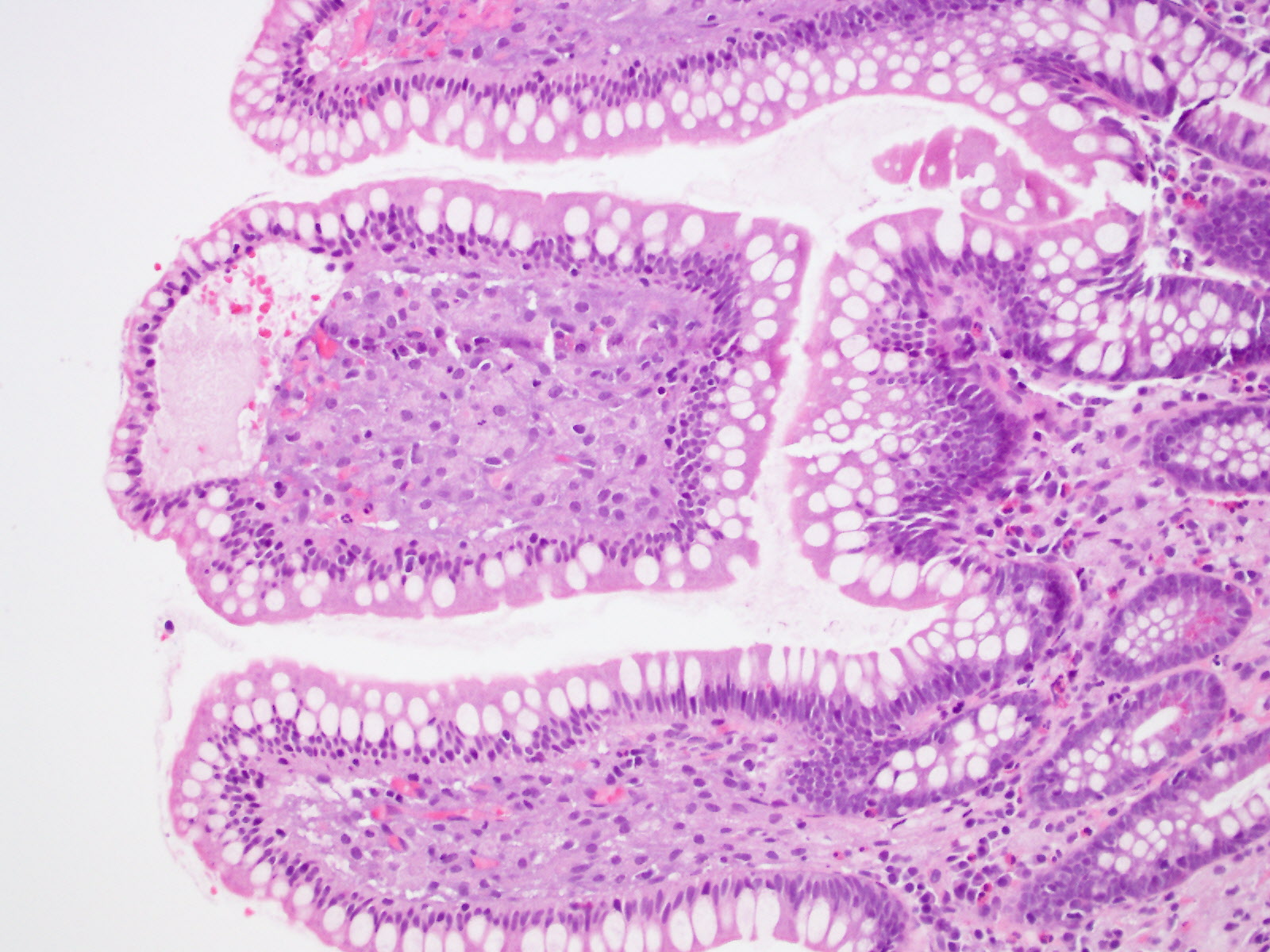
Figure: H&E stain from Terminal ileum, Duodenal and Ileal mucosa with lamina propria expansion by numerous foamy macrophages
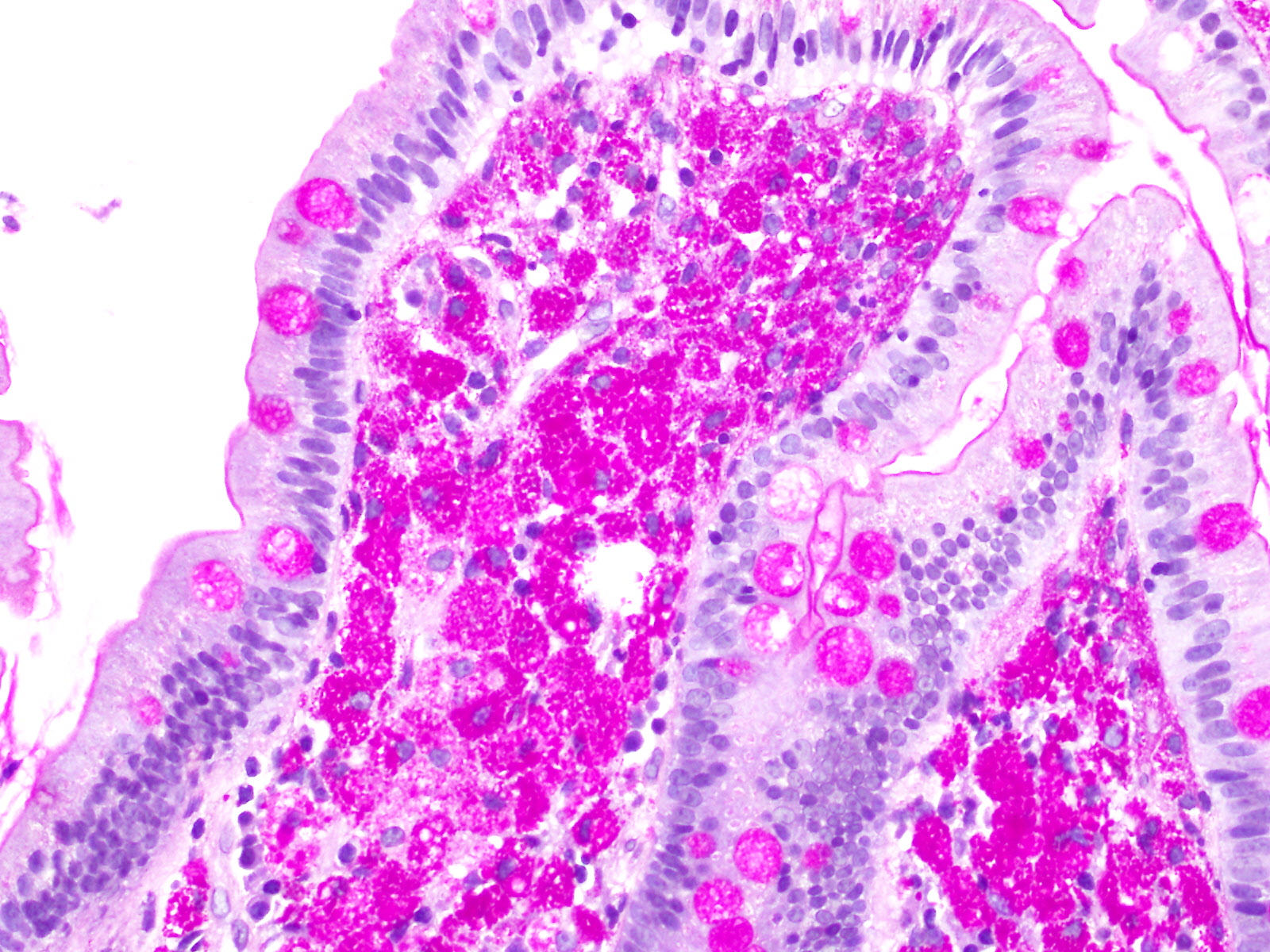
Figure: PAS stain - Foamy macrophages contain abundant PAS positive variably sized cytoplasmic inclusions.
Disclosures: Amit Rajkarnikar indicated no relevant financial relationships. Vy Luong indicated no relevant financial relationships. Alexandra Hebert indicated no relevant financial relationships. Melanie Bienvenu indicated no relevant financial relationships. Shantell Ceaser Ford indicated no relevant financial relationships. Christopher Wexler indicated no relevant financial relationships.
Amit Rajkarnikar, MD1, Vy Luong, DO1, Alexandra Hebert, MS2, Melanie Bienvenu, MD, MPH1, Shantell Ceaser Ford, MD1, Christopher Wexler, MD1. P1312 - When Common Symptoms Hide Rare Diseases: A Case of Prolonged Arthralgia and Chronic Diarrhea Unveiled as Whipple’s Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")