P1382 - Intraprocedural Real-Time Predictors of Failure in Patients With Roux-en-Y Gastric Bypass Undergoing Double-Balloon Assisted ERCP: Is There an Optimal Time to Cross-Over to EUS-Directed Transgastric ERCP?
SUNY Upstate Medical University Hospital Syracuse, NY
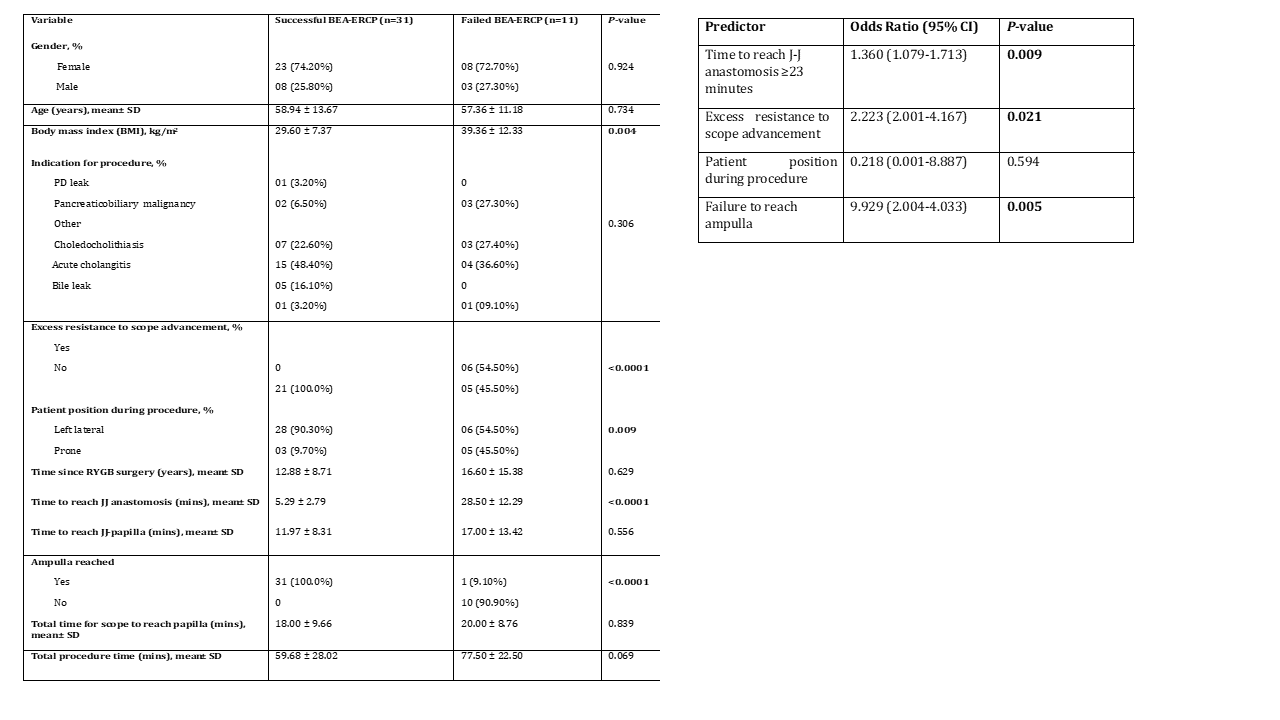
Azhar Hussain, MBBS1, Kambiz Khadkhodayan, MD2, Saurabh Chandan, MD3, Shayan S. Irani, MD4, Abdullah Abbasi, MD3, Mohamad Khaled Almujarkesh, MD2, Natalie Cosgrove, MD3, Deepanshu Jain, MD3, Maham Hayat, MD3, Zubair Khan, MD5, Sagar J.. Pathak, MD3, Mustafa Arain, MD3, Dennis Yang, MD, FACG6, Muhammad Hasan, MD, FACG3 1SUNY Upstate Medical University Hospital, Syracuse, NY; 2AdventHealth, Orlando, FL; 3Center for Interventional Endoscopy, AdventHealth Orlando, Orlando, FL; 4Virginia Mason Medical Center, Seattle, WA; 5Mercy Clinic East Communities, Festus, MO; 6Center for Interventional Endoscopic, AdventHealth Orlando, Orlando, FL Introduction: Double-balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography (BEA-ERCP) is a common approach for managing pancreaticobiliary disease in patients with Roux-en-Y gastric bypass (RYGB). Our study aimed to identify intraprocedural predictors of BEA-ERCP failure and determine the optimal timing for cross-over to endoscopic ultrasound-directed transgastric ERCP (EDGE) during the same session. Methods: We prospectively evaluated consecutive RYGB patients undergoing BEA-ERCP from 2021 to 2024. Procedure-related data was collected prospectively, and patients were divided into two cohorts based on procedure outcome: patients with successful versus failed BEA-ERCP. Binary logistic regression analyses were conducted to identify intraprocedural predictors of BEA-ERCP failure. Receiver operating characteristic (ROC) curves were used to determine the optimal timing for cross-over to EDGE. Results: Forty-two patients (11 males, 31 females) underwent BEA-ERCP with a success rate of 73.8% (n=31). Significant risk factors of BEA-ERCP failure included excessive resistance to scope advancement (P< 0.0001), failure to reach the ampulla (P< 0.0001), patient position (P=0.009), BMI (P=0.004) and time to reach the jejuno-jejunal (J-J) anastomosis (P< 0.0001). Binary logistic regression analysis identified time to reach the J-J anastomosis ≥23 minutes [OR 1.360 (95% CI:1.079-1.713), P=0.009], excess resistance to scope advancement [OR 2.223 (95% CI: 2.001-4.167)] and failure to reach ampulla [OR 9.929 (95% CI: 2.004-4.033)] as the statistically significant predictors of BEA-ERCP failure (Table 1). When there were ≥2 predictors of BA-ERCP failure, the likelihood of having failed BA-ERCP was 2.370 with 95.50% sensitivity and 90% specificity with AUC= 0.929 (p=0.0001). Discussion: Time to reach the J-J anastomosis of ≥23 minutes, excess resistance to scope advancement, and failure to reach the ampulla are significant predictors of BEA-ERCP failure. When there were ≥2 predictors of BA-ERCP failure present, it represents an optimal time to cross over to EDGE. These findings can guide clinical decision-making and improve procedural outcomes.
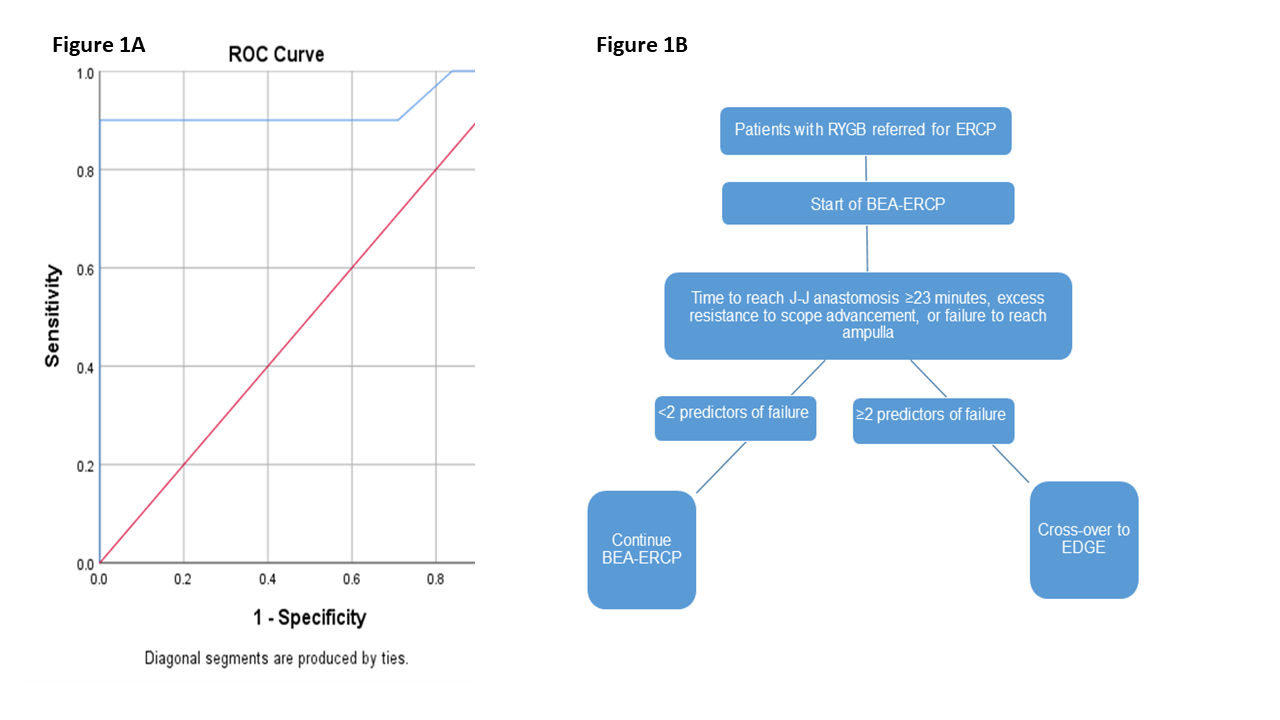
At our institution, after obtaining consent for both BAE-ERCP and EDGE, all patients with uncomplicated pancreaticobiliary disease undergo BAE-ERCP first. If the J-J is not reached within 23 minutes, endoscopist is experiencing excessive scope resistance and/or ampulla is not reached altogether, an early decision is made to cross over to EDGE (Fig 1).
Figure: Table 1: Baseline clinical characteristics, procedural parameters (left), and predictors of BEA-ERCP failure (right) on binary logistic regression analysis
Figure: Figure 1: (1A) ROC curve for predicting failure based on ≥2 predictors of BA-ERCP failure. (1B) Algorithm used for ERCP in RYGB patients with uncomplicated pancreaticobiliary disease.
Disclosures: Azhar Hussain indicated no relevant financial relationships. Kambiz Khadkhodayan indicated no relevant financial relationships. Saurabh Chandan indicated no relevant financial relationships. Shayan Irani: Boston Scientific – Consultant. ConMed – Consultant. W.L. Gore – Consultant. Abdullah Abbasi indicated no relevant financial relationships. Mohamad Khaled Almujarkesh indicated no relevant financial relationships. Natalie Cosgrove indicated no relevant financial relationships. Deepanshu Jain indicated no relevant financial relationships. Maham Hayat indicated no relevant financial relationships. Zubair Khan indicated no relevant financial relationships. Sagar Pathak indicated no relevant financial relationships. Mustafa Arain: Boston Scientific – Consultant. Cook Endoscopy – Consultant. Olympus – Consultant. Dennis Yang: 3D-Matrix – Consultant. Apollo Endosurgery – Consultant. ERBE – Consultant. Fujifilm – Consultant. Medtronic – Consultant. MicroTech – Consultant. Olympus – Consultant. Muhammad Hasan: Boston Scientific – Consultant. MicroTech Endoscopy – Consultant. Olympus America – Consultant.
Azhar Hussain, MBBS1, Kambiz Khadkhodayan, MD2, Saurabh Chandan, MD3, Shayan S. Irani, MD4, Abdullah Abbasi, MD3, Mohamad Khaled Almujarkesh, MD2, Natalie Cosgrove, MD3, Deepanshu Jain, MD3, Maham Hayat, MD3, Zubair Khan, MD5, Sagar J.. Pathak, MD3, Mustafa Arain, MD3, Dennis Yang, MD, FACG6, Muhammad Hasan, MD, FACG3. P1382 - Intraprocedural Real-Time Predictors of Failure in Patients With Roux-en-Y Gastric Bypass Undergoing Double-Balloon Assisted ERCP: Is There an Optimal Time to Cross-Over to EUS-Directed Transgastric ERCP?, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.