Allison Franz, MD1, Nanlong Liu, MD2 1University of Louisville, Louisville, KY; 2University of Louisville Division of Gastroenterology, Hepatology, and Nutrition, Louisville, KY Introduction: Bouveret’s syndrome is a rare complication of cholelithiasis, in which a large gallstone erodes into the proximal duodenum, creating a cholecystoduodenal fistula, and lodging itself immediately distal to the pyloric channel leading to a gastric outlet obstruction (GOO). It is most common in women with a history of gallstones, and typically presents with diffuse abdominal pain, nausea and vomiting. A radio-opaque obstruction of the proximal duodenum on imaging raises suspicion for Bouveret's syndrome. Treatment options include endoscopic, laparoscopic and open surgical intervention.
Case Description/
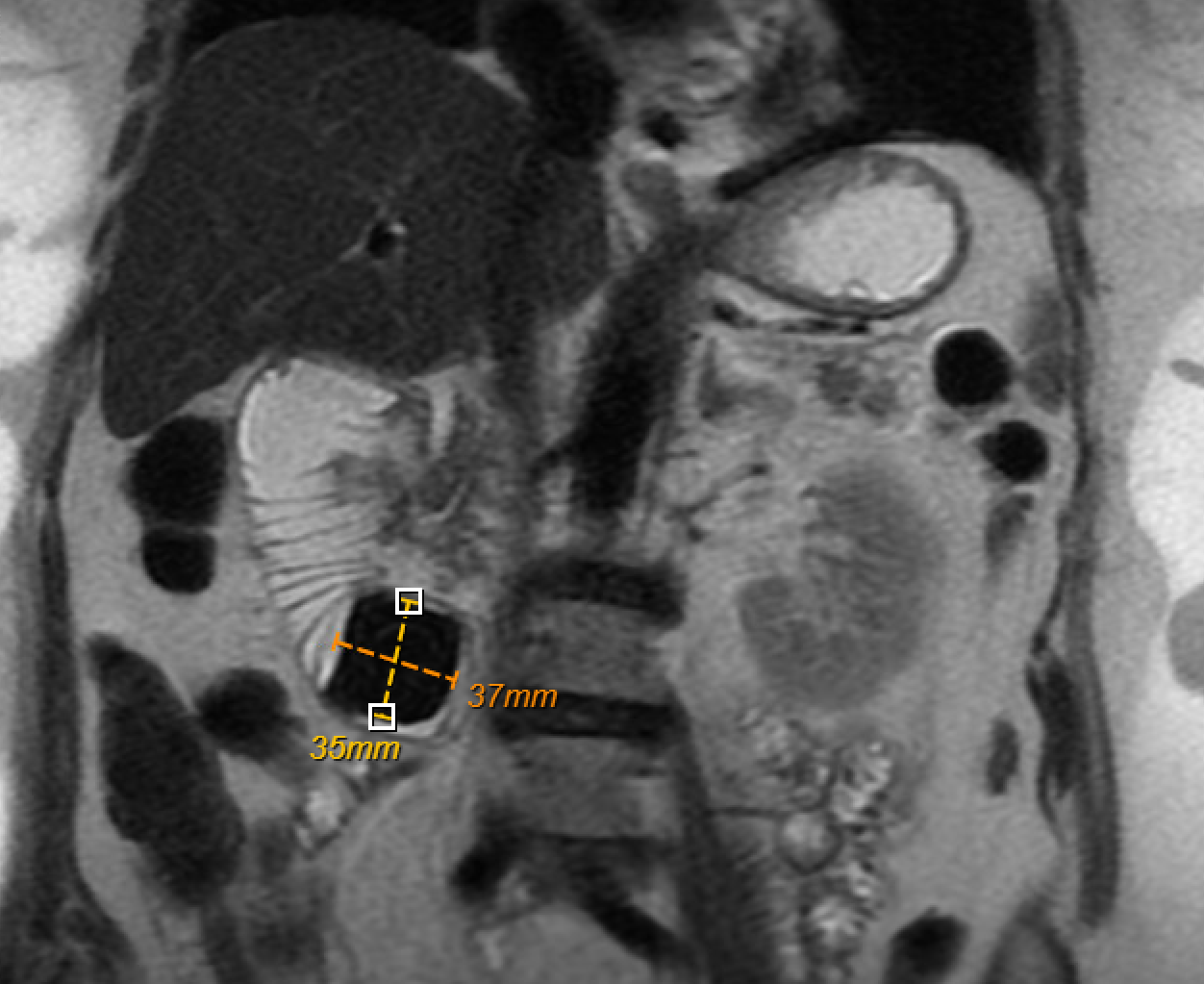
Methods: 77-year-old female presented with a 6-week history of nausea, vomiting and abdominal pain. Labs were notable only for elevated lipase (2500 U/L) with all other liver function tests within normal limits. CT of the abdomen showed a large mass in the proximal duodenum with evidence of pancreatitis and gastritis. MRCP confirmed a 3-cm gallstone in the duodenal bulb with cholecystoduodenal fistula, pneumobilia and evidence of complete GOO (fig 1). A nasogastric tube was placed, and multiple liters of gastric fluid were suctioned. The patient underwent EGD with ERCP for further evaluation with plan for bile duct stenting to aid with decompression in anticipation of need for surgical intervention with exploratory laparotomy. During EGD, meticulous fragmentation with electrohydraulic lithotripsy (EHL) was performed using 15 EHL probes. The stone was found to have three separate layers: an outer layer with green/black deposit, a yellow cholesterol layer and a very hard crystal-like core (fig 2). After three hours of EHL, the stone was successfully broken up with follow up CT confirming the presence of the fragments distally in the ascending colon. The patient recovered without complications and was discharged home a few days later without the need for surgical intervention Discussion: Bouveret’s syndrome is a rare cause of GOO characterized by cholecystoduodenal fistula complicated by large gallstone impaction within the enteric tract. There are currently no standardized guidelines for the management of Bouveret’s syndrome. Traditional management includes laparoscopic or open surgical stone removal, with individualized decision for subsequent cholecystoduodenal fistula repair and/or cholecystectomy. Advanced EGD techniques including mechanical removal and EHL allow patients to avoid the morbid risks associated with surgery.
Figure: Figure 1. MRCP showing the obstructing gallstone in the proximal duodenum with pneumobilia present.
Figure: Figure 2. Endoscopic view of fragmented gallstone clearly depicting the three separate layers: the dark outer layer, the yellow cholesterol layer and the crystal-like inner core.
Disclosures: Allison Franz indicated no relevant financial relationships. Nanlong Liu indicated no relevant financial relationships.
Allison Franz, MD1, Nanlong Liu, MD2. P1464 - Bouveret’s Syndrome: A Rare Form of Gallstone Ileus, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")