Neal K. Bhachawat, DO1, Apaar Dadlani, MD1, Heather L. Stevenson, MD, PhD2, Adeel Shahid, MD1, Sudha Kodali, MD1 1Houston Methodist Hospital, Houston, TX; 2UTMB, Galveston, TX Introduction: Budd-Chiari syndrome (BCS) is rare and usually presents with hepatomegaly, abdominal pain, transudative ascites and volume overload. Delayed diagnosis may lead to acute liver failure or cirrhosis. Given its implications, clinicians must consider BCS in atypical presentations. We present a rare case of recurrent exudative pleural effusions as the initial manifestation of BCS—the first reported, to our knowledge.
Case Description/
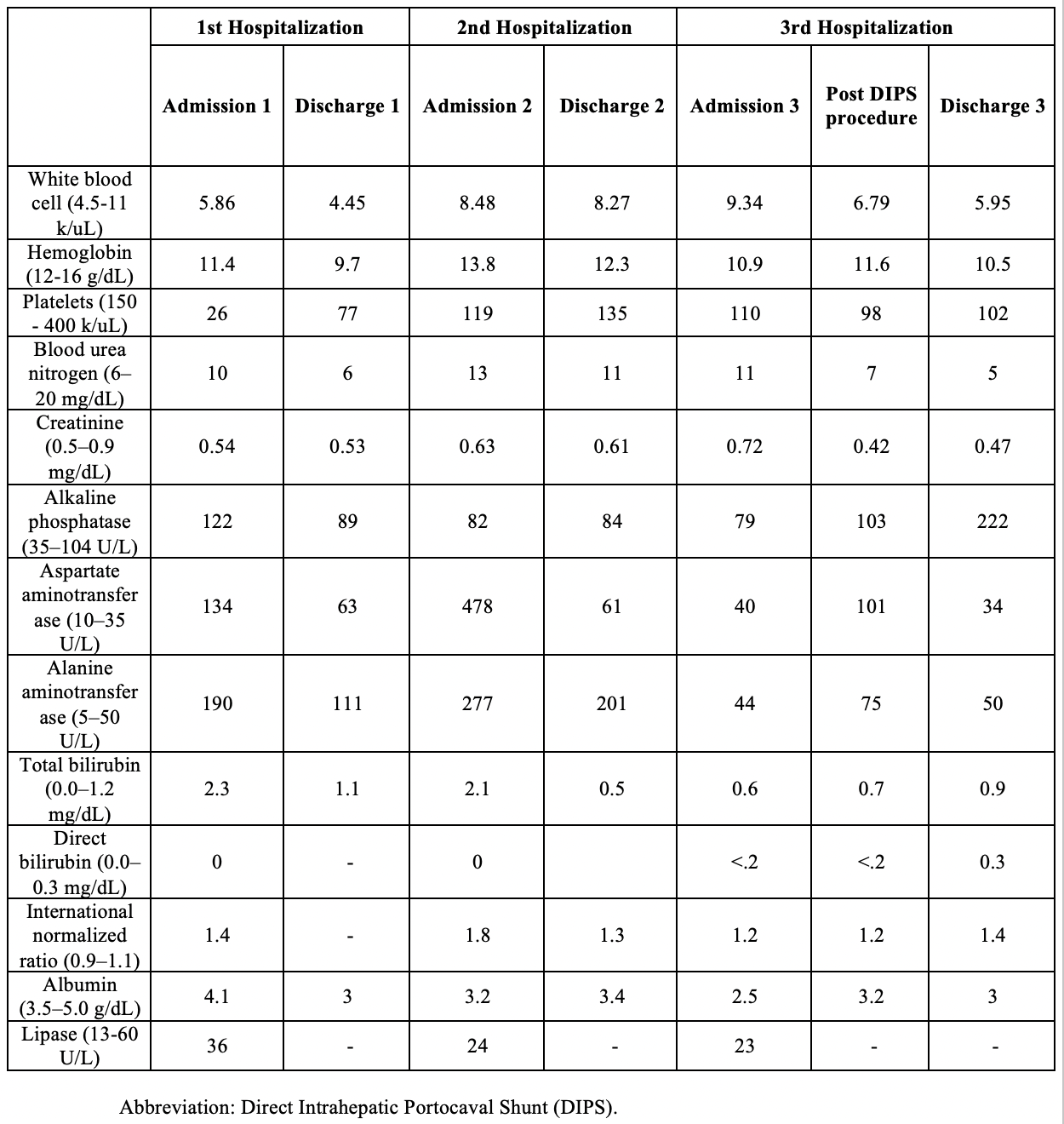
Methods: 18-year-old African American female with no PMH presented with dyspnea. She noted recent travel to California and Kentucky, and a possible tick bite. Exam noted right-sided decreased breath sounds and dullness to percussion. CT scan showed moderate ascites, bilateral pleural effusions (right >left), and heterogeneous liver attenuation. Liver enzymes elevated in hepatocellular pattern (table 1-hospital 1); workup was negative for viral, autoimmune, and genetic causes. Paracentesis with SAAG >1.1 g/dl suggestive of a post-sinusoidal etiology. Diagnosed with acute hepatitis possibly due to a tick-borne illness, she was discharged on doxycycline. 11 days later, she re-presented with similar symptoms, worsening liver tests(table 1-hospital 2) and pleural effusions. Thoracentesis revealed exudative fluid; cultures negative. Liver biopsy showed sinusoidal dilatation and perivenular necrosis. She was suspected to have doxycycline induced liver injury and the drug was stopped. 9 days later, she presented for worsening dyspnea. Labs showed improved liver enzymes (table 1-hospital 3). She required chest tube placement for persistent exudative pleural effusions. Hepatic venogram revealed a portal gradient of 17 mmHg (normal< 5 mmHg), a severely stenotic left hepatic vein, and non-catheterizable right hepatic vein—findings consistent with BCS. She underwent direct intrahepatic portosystemic shunt (DIPS) placement (image 2) on day 31 of hospitalization. Bone marrow biopsy revealed diagnosis of Paroxysmal Nocturnal Hemoglobinuria and she was treated with eculizumab. Following DIPS, she had resolution of her symptoms. Discussion: The mechanism of pleural effusions in BCS is not well understood. While transudative effusions have been reported, exudative effusions have not. This case highlights an unusual presentation of BCS with refractory exudative pleural effusions, ultimately responsive to DIPS. It underscores the need to maintain a high index of suspicion for BCS, especially in young women with unexplained fluid overload, to avoid diagnostic delay and long-term complications.
Figure: Lab work from Hospitalization 1 – 3
Figure: Final direct intrahepatic portosystemic shunt (DIPS) procedure with successful tract creation between portal vein and inferior vena cava
Disclosures: Neal Bhachawat indicated no relevant financial relationships. Apaar Dadlani indicated no relevant financial relationships. Heather Stevenson indicated no relevant financial relationships. Adeel Shahid indicated no relevant financial relationships. Sudha Kodali: ASTRAZENECA – Advisory Committee/Board Member. GILEAD – Advisor or Review Panel Member, Advisory Committee/Board Member, Speakers Bureau. SIRTEX – Advisor or Review Panel Member.
Neal K. Bhachawat, DO1, Apaar Dadlani, MD1, Heather L. Stevenson, MD, PhD2, Adeel Shahid, MD1, Sudha Kodali, MD1. P1718 - Recurrent Exudative Pleural Effusions as Initial Presentation for Budd-Chiari Syndrome (BCS), ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.