Washington Township Medical Group Mountain View, CA
Hiba Ghannam, MD1, Abdulhadi Abo Nofal, 2, Keenan Kassar, MBA3, Zaid Imam, MD4 1Health Point Abudhabi, Abudhabi, Abu Dhabi, United Arab Emirates; 2Alfaisal University, Riyadh, Ar Riyad, Saudi Arabia; 3Loyola University, Lemont, IL; 4Washington Hospital Healthcare System, Mountain View, CA Introduction: Population prevalence rates of benign liver cysts range from 2.5-5% and are most commonly asymptomatic. We report a case of multiple symptomatic benign liver cysts presenting with chronic right upper quadrant discomfort, highlighting considering this as an etiology of abdominal pain after a thorough diagnostic work-up.
Case Description/
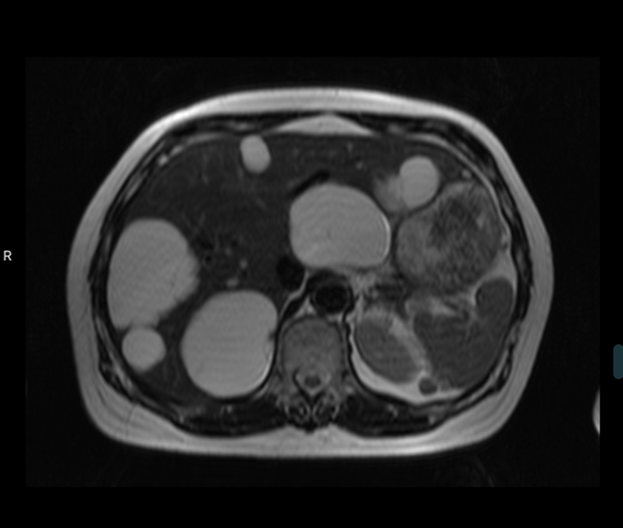
Methods: A 58-year-old-Asian female with no prior medical history presented for with right upper quadrant discomfort and early satiety for 5 years. She denied being involved in sheepherding or farming or living in rural areas. A complete blood count, liver enzyme panel, celiac serologies, and serum lipase were normal. Helicobacter Pylori breath testing was negative. A right upper quadrant ultrasound demonstrated multiple liver cysts, the largest was 8 cm and no biliary pathology. She received an 8-week trial of proton pump inhibitor therapy with two different agents with no benefit. An esophagogastroduodenoscopy was normal. Gastric biopsies for H. Pylori testing were negative. She denied non-steroidal anti-inflammatory medication use. A magnetic resonance imaging (MRI) of the abdomen was performed, demonstrating numerous liver cysts, the largest at segments 6/7 measuring 7.5 x 6.1 cm and 8.6 x 5.3 cm respectively (Image 1). No renal cysts were observed. No biliary pathology was identified. A CT guided aspiration of the three largest cysts was performed providing temporary pain relief following the procedure but presented 2 weeks later with worsening abdominal pain. Repeat imaging did not demonstrate subcapsular hemorrhage or intra-cystic hemorrhage. She was treated conservatively and discharged home with surgical follow-up. Two months later, she underwent a laparoscopic fenestration of multiple hepatic cysts focusing on the cysts closest to her stomach and larger right sided cysts. A total of 8 cysts were fenestrated. The anatomic pathology specimens demonstrated thick fibrous walled cysts with bland cuboidal epithelium consistent with benign liver cysts. No infectious pathogens were identified. She was seen a month later resolution of her presenting symptoms. Discussion: This case highlights a common incidental liver pathology that is rarely symptomatic. After a thorough work-up excluding other differential diagnosis, addressing the cysts with laparoscopic fenestration yielded an excellent result with relief of the patient’s symptoms. This highlights the importance of recognizing larger benign liver cysts as a possible etiology of abdominal discomfort.