California Pacific Medical Center San Francisco, CA
Torrey Y. Czech, , Thomas Y. Myint, California Pacific Medical Center, San Francisco, CA Introduction: Hepatocellular carcinoma (HCC) is the fourth most common cause of cancer-related mortality globally and the leading cause of death in patients with cirrhosis.
Advancements in the management of late-stage HCC include immunotherapy, surgery, and locoregional therapy (LRT) in combination with systemic therapy.
Case Description/
Methods: An 83-year old Chinese-American male with history of HCC s/p right hepatectomy (8/2018) presented to the emergency department with hematochezia.
On admission he was found to have a hemoglobin of 13.6 (1/2/25), platelets of 169, and INR of 1.0. A CT scan demonstrated uncomplicated colonic diverticulosis and long-segment sigmoid wall thickening. Colonoscopy the following day demonstrated a hemorrhagic 3.5 cm polyp in the sigmoid colon. Polypectomy was performed as it was the presumed source of bleeding. On pathology the polyp showed metastatic hepatocellular carcinoma.
The patient has a history of E antigen negative chronic hepatitis B with HBsAg seroclearance and anti-HBs production and negative HBV DNA. He was on entecavir May 2018 with complete virologic response and was aviremic post therapy. His history of HCC was notable for moderately differentiated 8.1 cm tumor in segment 5 with microvascular invasion, s/p hepatectomy August 2018 with negative margins.
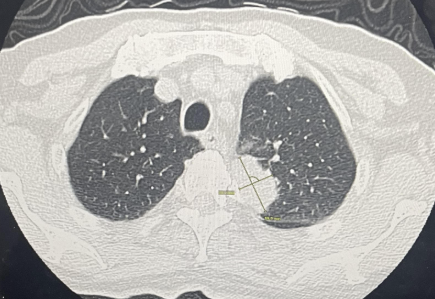
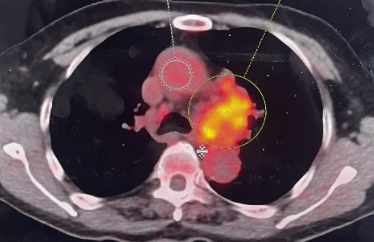
A PET/CT scan revealed mediastinal metastases, a left upper lung mass, left frontoparietal metastasis and right occipital lobe metastasis. He underwent left craniotomy. Pathology demonstrated metastatic HCC. He then underwent stereotactic radiosurgery to right occipital metastatic lesion. The patient has been started on atezolizumab and bevacizumab. Discussion: This case demonstrates an unusual presentation of advanced HCC in a patient with hematochezia six years following right hepatectomy and HBV e antigen seroconversion.
Other causes of malignancy were excluded based on pathology report however our leading suspicion given a hemorrhagic appearing polyp included colorectal adenocarcinoma.
Despite a right hepatectomy with negative margins, it is likely that the patient developed metastatic disease due to the microvascular invasion. While the patient had serial normal alpha-fetoprotein and negative cross-sectional abdominal imaging, this presentation of metastatic disease was atypical and severe at time of diagnosis given hematochezia, lung, mediastinal and intracranial involvement. This case highlights the importance of continued close monitoring of patients with a history of HCC status post resection.
Figure: PET/CT with metastatic lesion of left upper lobe
Figure: PET/CT with mediastinal involvement
Disclosures: Torrey Czech indicated no relevant financial relationships. Thomas Myint indicated no relevant financial relationships.
Torrey Y. Czech, , Thomas Y. Myint, . P1787 - An Atypical Presentation of Metastatic Hepatocellular Carcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.