Lakeland Regional Health Medical Center Lakeland, FL
Amanda Rigdon, MD1, Omar Zuhdi, MD1, Camila Villacreses, DO1, Brian Byun, DO2, Sanjiv Gray, MD1 1Lakeland Regional Health Medical Center, Lakeland, FL; 2Lakeland Regional Health, Lakeland, FL Introduction: Umbilical hernias occur in 20% of patients with cirrhosis and ascites, with surgical management presenting significant challenges due to increased perioperative morbidity and mortality. The optimal timing and approach for hernia repair in decompensated cirrhosis remains controversial.
Case Description/
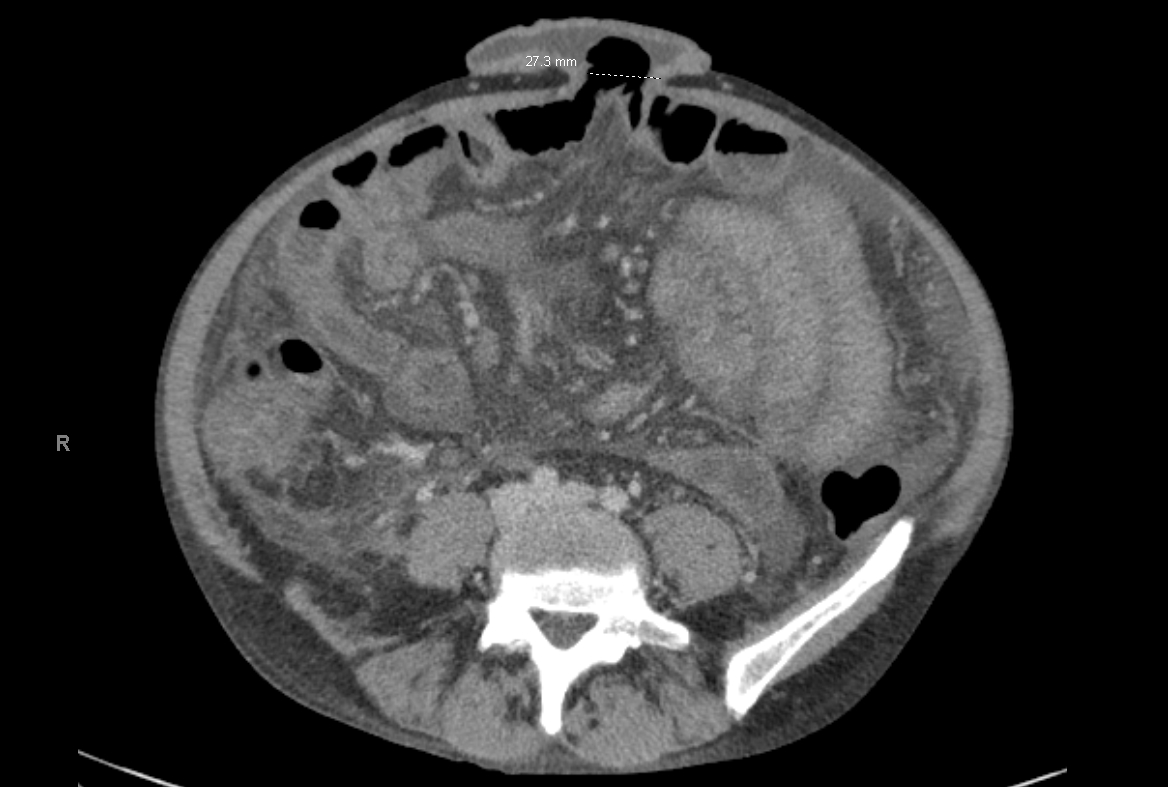
Methods: A 48-year-old male with no known medical history presented with worsening abdominal pain and draining umbilical hernia. He reported consuming 8-10, 32-ounce beers weekly. Physical examination revealed a 2.7 cm umbilical hernia with fluid-filled sac and intermittent drainage. Laboratory findings demonstrated severe anemia (hemoglobin 4.9 g/dL), thrombocytopenia (platelet count 73,000/μL), leukopenia (WBC 3,000/μL), coagulopathy (INR 1.6), hyponatremia, hypokalemia, and hyperammonemia. CT imaging revealed cirrhosis with ascites, portal hypertension, and gallbladder edema. Fecal occult blood testing was positive.
During hospitalization, the patient was newly diagnosed with alcoholic liver cirrhosis with a MELD-Na score of 22. Esophagogastroduodenoscopy (EGD) performed on hospital day 2 revealed esophageal varices, gastroparesis, and gastritis. Initial paracentesis yielded 2,750 cc of ascitic fluid with 92% segmented neutrophils but negative for spontaneous bacterial peritonitis. A second paracentesis on hospital day 3 removed 650 cc of clear fluid.
Following medical optimization with diuretics (spironolactone 100 mg daily, furosemide 40 mg daily), propranolol for varices prophylaxis, and pantoprazole for gastroprotection, the patient underwent successful umbilical hernia repair. Post-operative management included continued ascites control through diuretic optimization rather than serial paracentesis, as recommended by interventional radiology given minimal fluid reaccumulation. Discussion: This case illustrates the complex management of umbilical hernia in newly diagnosed decompensated cirrhosis. Key considerations include preoperative risk stratification using MELD score, optimization of medical management including ascites control, and careful patient selection. The risk of persistent drainage from surgical sites due to ongoing portal hypertension was discussed extensively with the patient preoperatively. Our approach emphasized medical optimization over aggressive paracentesis, consistent with current guidelines recommending diuretic therapy as first-line treatment for ascites management.