Harnoor Brar, MS, Kirandeep Kaur, , Ujagger Dhillon, MD, FACG, Gurjiwan Virk, MD, Amandeep Sandhu, RN, NP, JayaKrishna Chintanaboina, MD, MPH California Digestive Disease Center, Fresno, CA Introduction: Wilson’s disease is a rare autosomal recessive disorder of copper (Cu) metabolism caused by mutations in the ATP7B gene, leading to impaired biliary Cu excretion and accumulation in the liver, brain, and cornea. Hepatic steatosis is an early sign, especially in young patients, and can mimic metabolic dysfunction-associated steatohepatitis (MASH), which can often lead to delayed diagnosis. We present a case of Wilson’s Disease in a young male who was initially misdiagnosed with MASH.
Case Description/
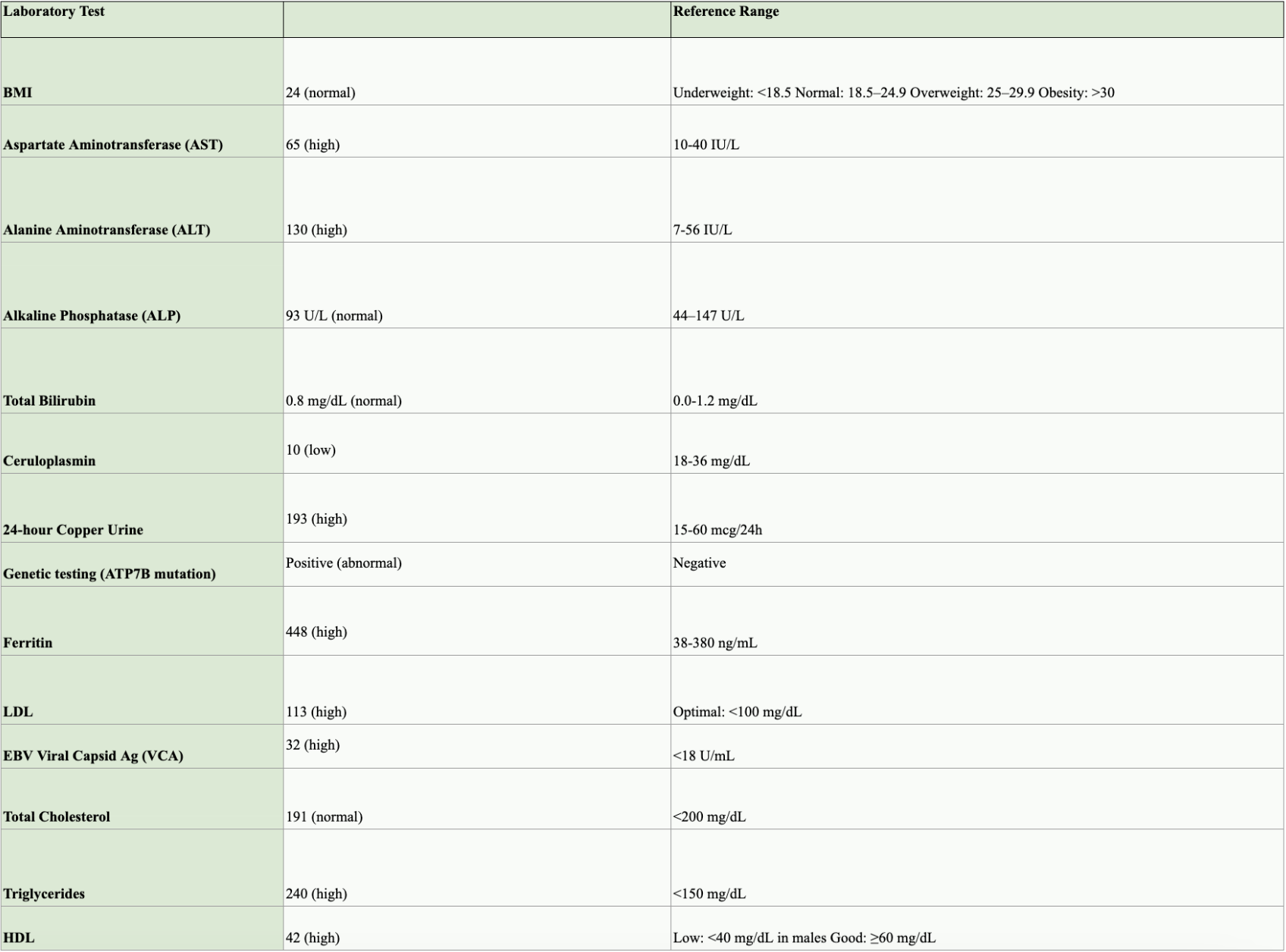
Methods: A 28-year-old Asian male with no significant medical history was incidentally found to have elevated transaminases (Table 1) during an annual exam. His BMI was 24, and he had no risk factors for metabolic syndrome or alcoholic liver disease. He was initially diagnosed with MASH based on hepatic steatosis seen on ultrasound. He was later referred to us after he moved out of state.
Physical examination was unremarkable. Laboratory data showed low ceruloplasmin (Table 1) concerning Wilson's Disease. MRI liver demonstrated diffuse hepatic steatosis. FibroScan showed minimal fibrosis (5.0 kPa, F0–1) with steatosis of 295 dB/m and S1. A liver biopsy showed severe steatosis without ballooning or fibrosis. Although the qualitative Cu was negative, a very high quantitative Cu, 1008 mcg/g dry wt ( < 50 mcg/g dry wt), and 24-hour urinary copper excretion confirmed Wilson’s disease (Table 1). Genetic testing for ATP7B was positive. A Slit-lamp exam was negative for Kayser-Fleischer rings. He was started on Trientine HCl (500 mg AM & 750 mg PM). Discussion: Our case underscores the complexity of diagnosis of Wilson's disease when hepatic steatosis is the only prominent finding. Differential diagnoses other than MASH should be considered in the workup of hepatic steatosis (Table 2). Kayser-Fleischer rings may not be seen during the early course of the disease. Qualitative Cu stains on liver biopsy alone can be unreliable due to uneven Cu distribution. Quantitative hepatic Cu ( >250 mcg/g dry wt) and elevated urinary Cu excretion remain essential diagnostic tools. A broader differential, including Wilson’s disease, should be considered in younger adults with elevated liver enzymes, even when imaging suggests MASH. Early diagnosis through comprehensive Cu studies allows for timely chelation therapy, helping to prevent irreversible liver or neurologic damage.
Figure: Table 1: Laboratory Report
Figure: Table 2: Differential Diagnosis of Steatosis
Disclosures: Harnoor Brar indicated no relevant financial relationships. Kirandeep Kaur indicated no relevant financial relationships. Ujagger Dhillon indicated no relevant financial relationships. Gurjiwan Virk indicated no relevant financial relationships. Amandeep Sandhu indicated no relevant financial relationships. JayaKrishna Chintanaboina indicated no relevant financial relationships.
Harnoor Brar, MS, Kirandeep Kaur, , Ujagger Dhillon, MD, FACG, Gurjiwan Virk, MD, Amandeep Sandhu, RN, NP, JayaKrishna Chintanaboina, MD, MPH. P1868 - Wilson’s Disease Initially Misdiagnosed as Metabolic Dysfunction-Associated Steatohepatitis in a Young Male, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.