Reeti Gulati, MD1, Ugochukwu Akpara, MD1, Averie Dickinson, MD1, Isaac Smith, MD2, Matthew Kappus, MD3 1Duke University School of Medicine, Durham, NC; 2Division of Rheumatology and Immunology, Duke University School of Medicine, Durham, NC; 3Division of Gastroenterology, Duke University School of Medicine, Durham, NC Introduction: Hereditary hemochromatosis (HH) is an iron overload disorder caused by hemostatic iron regulator (HFE) gene mutations. In White European populations, over 90% of cases involve C282Y homozygosity, while 2-7% involve C282Y/H63D compound heterozygosity. We report a case of HH with compound heterozygosity presenting as inflammatory polyarthritis.
Case Description/
Methods: A 47-year-old White male with history of hypertension presented with 2 weeks of progressive inflammatory polyarthritis involving his left ankle, left wrist, left elbow, and bilateral knees, leading to immobility. He also had a history of recurrent bilateral knee pain requiring steroid injections. Joint x-rays showed diffuse chondrocalcinosis. Labs revealed liver injury (AST 69, ALT 156, total bilirubin 2.0, ALP 210, and INR 1.4) without alcohol use. He underwent serologic work-up, arthrocentesis, imaging, and biopsy to evaluate the etiology. Serologic work-up revealed leukocytosis (14.4), elevated ESR ( >130 mm/hr), CRP (30.71 mg/dL), and ferritin of 2561 with normal transferrin saturation (32%). Rheumatoid factor (13) and IgA (582) were mildly elevated; other infectious and autoimmune tests were negative. Arthrocentesis attempts yielded minimal fluid without bacteria or crystals. Medical records revealed elevated ferritin (745) and AST (43) nine years prior. HFE mutation analysis at that time identified the patient as a compound heterozygote for C282Y and H63D mutations. Repeat mutation analysis confirmed prior results. Liver biopsy during admission showed diffuse 1+ to 2+ hepatocyte iron deposition concerning for HH (Figure 1). Calcium pyrophosphate deposition disease (CPPD) was concluded to be the cause of his inflammatory polyarthritis given presence of chondrocalcinosis on x-rays (Figure 2). Despite treatment with prednisone, colchicine, and anakinra, symptoms persisted until high-dose IV methylprednisone was added. His very resistant CPPD arthritis suggested an underlying precipitating factor, in this case HH. He was discharged on a prednisone taper and colchicine and initiated on phlebotomy treatments to lower ferritin below 100. Discussion: C282Y/H63D compound heterozygosity in HH has low penetrance with only 0.5-2% of patients exhibiting iron overload-related disease. We report a case where this genotype presented as severe, treatment-resistant CPPD. In patients with severe inflammatory polyarthritis and transaminitis, HH precipitating CPPD should be considered as early management can help prevent organ damage.
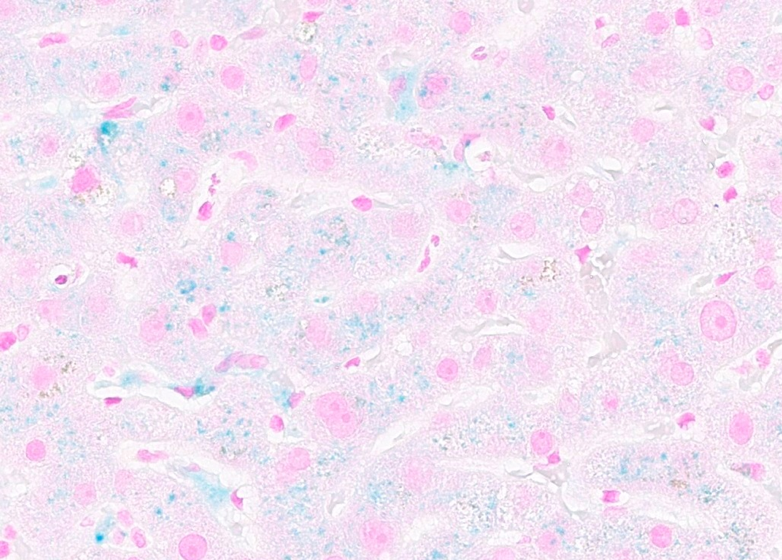
Figure: This slide from the patient’s liver biopsy demonstrates hepatocellular iron deposition along with focal Kupffer cell iron deposition (shown in blue) concerning for hereditary hemochromatosis.
Figure: Left wrist x-ray shows radiopaque punctate and linear densities within the patient’s radiocarpal and triangular fibrocartilage complex articular cartilage, representing chondrocalcinosis. Chondrocalcinosis was present on x-ray in many of his painful joints, supporting the diagnosis of CPPD.
Disclosures: Reeti Gulati indicated no relevant financial relationships. Ugochukwu Akpara indicated no relevant financial relationships. Averie Dickinson indicated no relevant financial relationships. Isaac Smith indicated no relevant financial relationships. Matthew Kappus indicated no relevant financial relationships.
Reeti Gulati, MD1, Ugochukwu Akpara, MD1, Averie Dickinson, MD1, Isaac Smith, MD2, Matthew Kappus, MD3. P1866 - Inflammatory Polyarthritis as the Initial Presentation of Hereditary Hemochromatosis with Compound Heterozygosity C282Y/H63D, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")