Reeti Gulati, MD1, Ugochukwu Akpara, MD1, Anna Mae Diehl, MD2 1Duke University School of Medicine, Durham, NC; 2Duke University Medical Center, Durham, NC Introduction: Sarcoidosis is a systemic granulomatous disease of unknown etiology. Hepatic involvement occurs in 50-65 percent of patients with sarcoidosis, although symptoms occur in only 5-15 percent. Rare case reports suggest that sarcoidosis may cause Budd Chiari syndrome. Here, we present a case of multi-organ sarcoidosis presenting as chronic Budd Chiari syndrome.
Case Description/
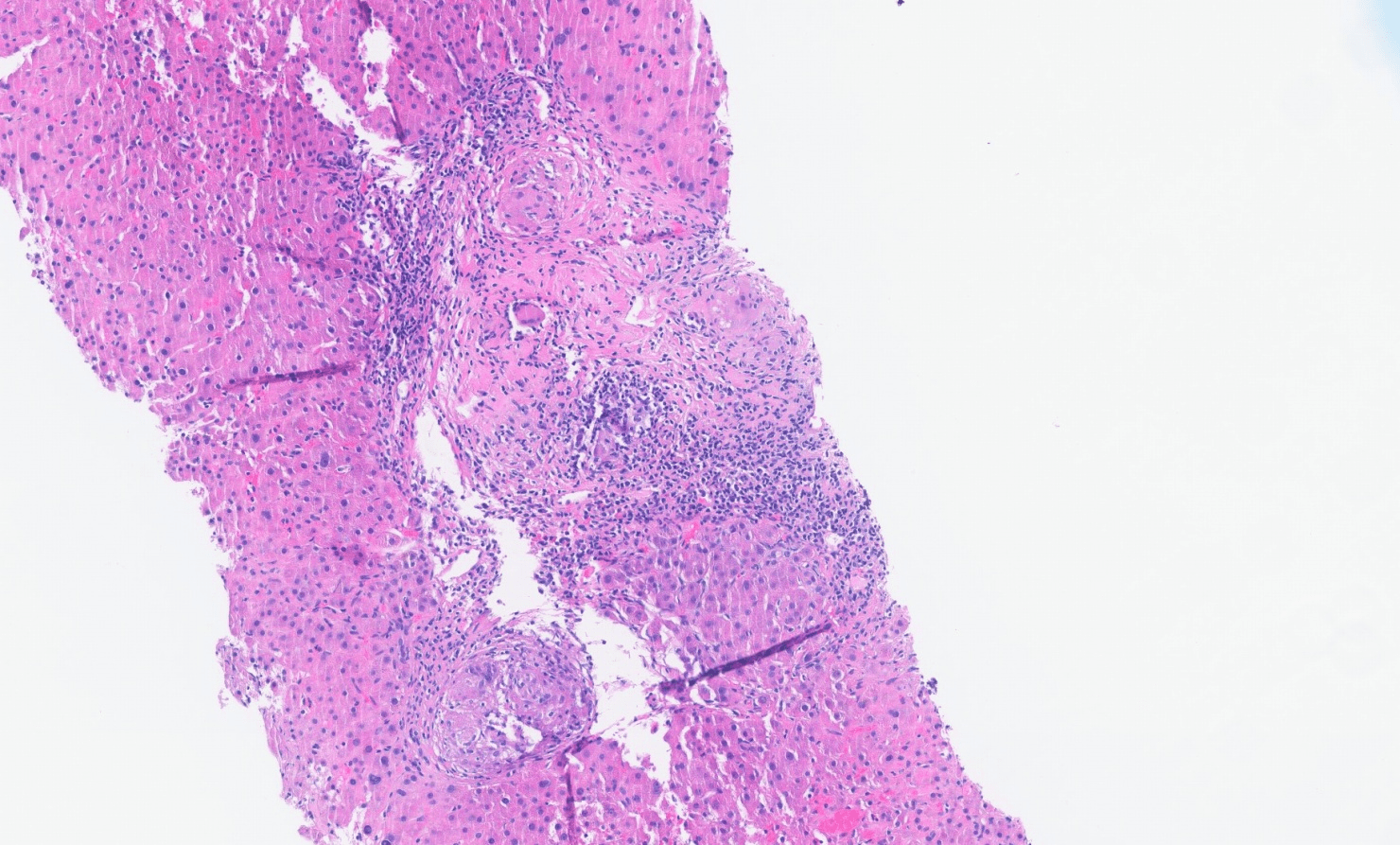
Methods: A 69-year-old, African-American male with no past medical history presented with dyspnea. He was found to have a hydropneumothorax along with liver injury of AST 110, ALT 67, total bilirubin 3.2, ALP 271, and INR 1.5. He reported 1 alcoholic drink monthly. He underwent serologic work-up, liver imaging, and liver biopsy to determine etiology of liver injury. Serologic work-up revealed strongly positive ANA with titer 1:2560, IgG level elevated to 3190, and IgA level elevated to 1470. CT abdomen pelvis with contrast revealed cirrhotic liver morphology with dilated splenic varices and small volume ascites fluid. MRI abdomen with and without contrast revealed chronic thrombosis of the intrahepatic and main portal veins and hepatic veins suggestive of chronic Budd Chiari syndrome. Liver histology revealed mild to moderate portal chronic inflammation with well-formed granulomas, portal fibrosis, and patchy sinusoidal dilation consistent with hepatic sarcoidosis (Figure 1). No cirrhosis was seen on biopsy. Stains for fungi and acid fast bacilli were negative. His course was complicated by hypotension, bradycardia, and acute hypoxic respiratory failure. Right heart catheterization was consistent with mild pre-capillary pulmonary hypertension. CT chest revealed bilateral central predominant architectural distortion and traction bronchiectasis consistent with pulmonary sarcoidosis. MRI brain revealed irregular pachymeningeal thickening in right frontoparietal high convexity indicative of neurosarcoidosis. Discussion: Multisystem sarcoidosis was concluded to be the unifying diagnosis. He was started on infliximab and prednisone. His liver enzymes down-trended and he was discharged on a prednisone taper. Budd Chiari syndrome is a rare complication of hepatic sarcoidosis. The pathogenesis consists of granulomatous inflammation leading to venous thrombosis and obstruction. In the setting of Budd Chiari syndrome without clear etiology, sarcoidosis should be considered. Prompt recognition and treatment of multisystem sarcoidosis with glucocorticoids and immunosuppressive agents is important to prevent irreversible organ damage.
Figure: Figure 1. This slide from the patient’s liver biopsy demonstrates portal granulomas surrounded by lymphoplasmacytic inflammation indicating presence of hepatic sarcoidosis.
Disclosures: Reeti Gulati indicated no relevant financial relationships. Ugochukwu Akpara indicated no relevant financial relationships. Anna Mae Diehl indicated no relevant financial relationships.
Reeti Gulati, MD1, Ugochukwu Akpara, MD1, Anna Mae Diehl, MD2. P1865 - Chronic Budd-Chiari Syndrome as Unique Presentation of Multi-Organ Sarcoidosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")