Hospital Roosevelt / Gastri-k Guatemala City, San Marcos, Guatemala
Victoria Morales, 1, Ninoska Meléndez, 2, Abel Sanchez, MD, MSc3 1Gastroenterology and Digestive Endoscopy, Roosevelt Hospital, Guatemala., Guatemala City, Chimaltenango, Guatemala; 21. Gastroenterology and Endoscopy Unit, Hospital Roosevelt Guatemala, Guatemala City, Quetzaltenango, Guatemala; 3Hospital Roosevelt / Gastri-k, Guatemala City, San Marcos, Guatemala Introduction: Superior mesenteric artery (SMA) syndrome is an uncommon cause of proximal intestinal obstruction, with an incidence of 0.001-0.0052% and an age range between 15-95 years, frequently affecting women, adolescents, and the elderly. It presents with postprandial vomiting (50%), early satiety (30%), and abdominal pain (59%), secondary to extrinsic compression of the third portion of the duodenum in patients who have experienced significant weight loss. Diagnosis can be challenging. However, timely treatment can prevent various complications (severe malnutrition, ischemia, and/or intestinal perforation). When conservative management fails, treatment involves duodenojejunal anastomosis. We present the case of a young female patient with significant weight loss and CT findings of SMA, with resolution of symptoms upon weight gain and without complications
Case Description/
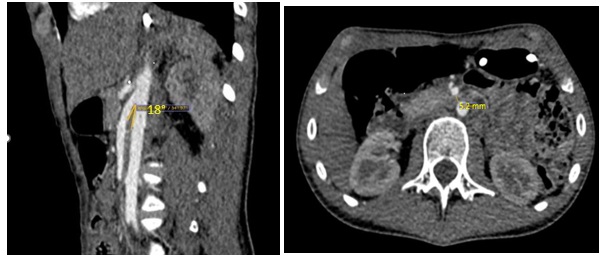
Methods: A 17-year-old Guatemalan female with a 6-month history of early satiety and vomiting of food content after each meal. She also reported intense epigastric pain without radiation and relief of symptoms with postural changes. She mentioned a weight loss of approximately 25 pounds. Upon evaluation, she was in very poor general condition, cachectic, with fine and brittle hair, generalized pallor, and a sunken abdomen with little subcutaneous tissue. Laboratory tests revealed mild anemia (Hb 10.2 mg/dL) and hypoalbuminemia (3.76 g/dL). She was admitted for nutritional support. Due to the emetic syndrome, an esophagogastroduodenoscopy was performed, revealing no abnormalities. A CT scan showed findings suggestive of gastrectasia, little subcutaneous tissue, an aorto-mesenteric angle of 18°, and an aorto-mesenteric distance of 5.2 mm. During her hospital stay, she was closely monitored by the nutrition team, gaining 12 pounds in 2 months and experiencing resolution of symptoms Discussion: Superior mesenteric artery syndrome is caused by extrinsic compression of the third portion of the duodenum, secondary to the loss of the intermediate mesenteric fat layer. The gold standard for diagnosis is evidence of a decreased aorto-mesenteric angle below 25° (normal 38-65°) and an aorto-mesenteric distance of less than 10 mm (normal 12-34 mm) by Angio CT, with a sensitivity of 42% and a specificity of 100%. The patient progressed satisfactorily with conservative treatment, i.e., weight gain with close monitoring by the nutrition team through a nasogastric tube and prokinetics, without presenting complications.
Figure: CT scan showed findings suggestive of gastrectasia, little subcutaneous tissue, an aorto-mesenteric angle of 18°, and an aorto-mesenteric distance of 5.2 mm
Disclosures: Victoria Morales indicated no relevant financial relationships. Ninoska Meléndez indicated no relevant financial relationships. Abel Sanchez indicated no relevant financial relationships.
Victoria Morales, 1, Ninoska Meléndez, 2, Abel Sanchez, MD, MSc3. P1947 - Superior Mesenteric Artery Syndrome: A Rare Cause of Emetic Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")