University of Florida Health Shands Hospital Gainesville, FL
Christopher A. Miquel-Chambers, MD1, Christiana M. Shaw, MD, MS1, Tiffany Chua, MD2 1University of Florida Health Shands Hospital, Gainesville, FL; 2University of Florida, Gainesville, FL Introduction: Angiosarcomas are exceedingly rare, constituting 2% of soft-tissue sarcomas[1] with a 30-50% recurrence rate at 5 years.[2]Gastrointestinal (GI) involvement, particularly the small bowel, is uncommon.
Case Description/
Methods: A 65-year-old male with a history of right neck angiosarcoma (treated with surgical excision and adjuvant chemotherapy and radiation in 2023 presented with acute right lower quadrant abdominal pain and fever in March 2025. His initial surveillance imaging for right neck angiosarcoma was negative. Workup of his new symptoms showed jejunal thickening and lymphadenopathy on CT, prompting referral to a tertiary care center. Small bowel enteroscopy revealed a friable, sessile jejunal lesion with central depression and ulceration. Biopsy results showed a poorly differentiated vascular neoplasm positive for ERG and CD31, consistent with angiosarcoma. The patient underwent resection: final surgical pathology showed metastatic epithelioid angiosarcoma involving the small bowel, with lymphovascular infiltration and one of eight lymph nodes positive for tumor. Genetic testing for 64 germline mutations was negative. Discussion: While primary angiosarcoma has a reported annual incidence of 3 per million in the U.S.[3], The incidence of metastatic small bowel angiosarcoma is not well-documented. Most literature involves case reports,[4] as large studies like the SEER database analysis of 284 metastatic angiosarcoma patients did not report small bowel involvement.[3]Primary small bowel angiosarcoma presenting as a bleeding mass has been reported, but metastatic cases are rare. The jejunum is an unusual site for metastases, as visceral angiosarcomas affect vascular-rich organs like the liver or spleen.[5]The most frequent sites of metastases are the lungs, liver, bones, and lymph nodes with the lungs being the predominant site, affected in 60.2% of metastatic cases[3]. Liver metastases are reported in 30.3% of cases, frequently characterized as multiple hypodense lesions with heterogenous involvement.
Clinical presentations vary by metastatic site. Hepatic metastases may present with abdominal pain or jaundice, and GI metastases manifest as pain, bleeding, or obstruction.[6-7]Our patient’s fever and acute pain suggest an inflammatory component, potentially complicating initial diagnosis. His non-specific presentation highlights the need to consider advanced diagnostic imaging and endoscopy in patients with a history of angiosarcoma.
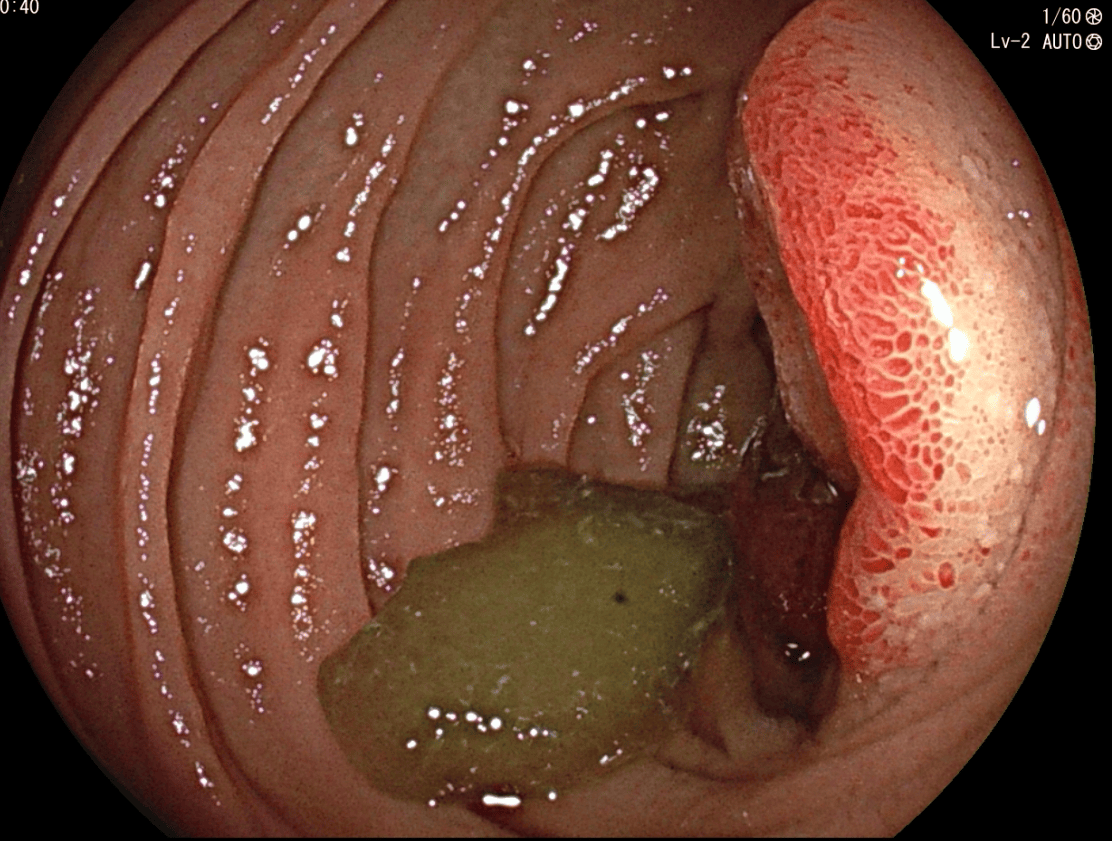
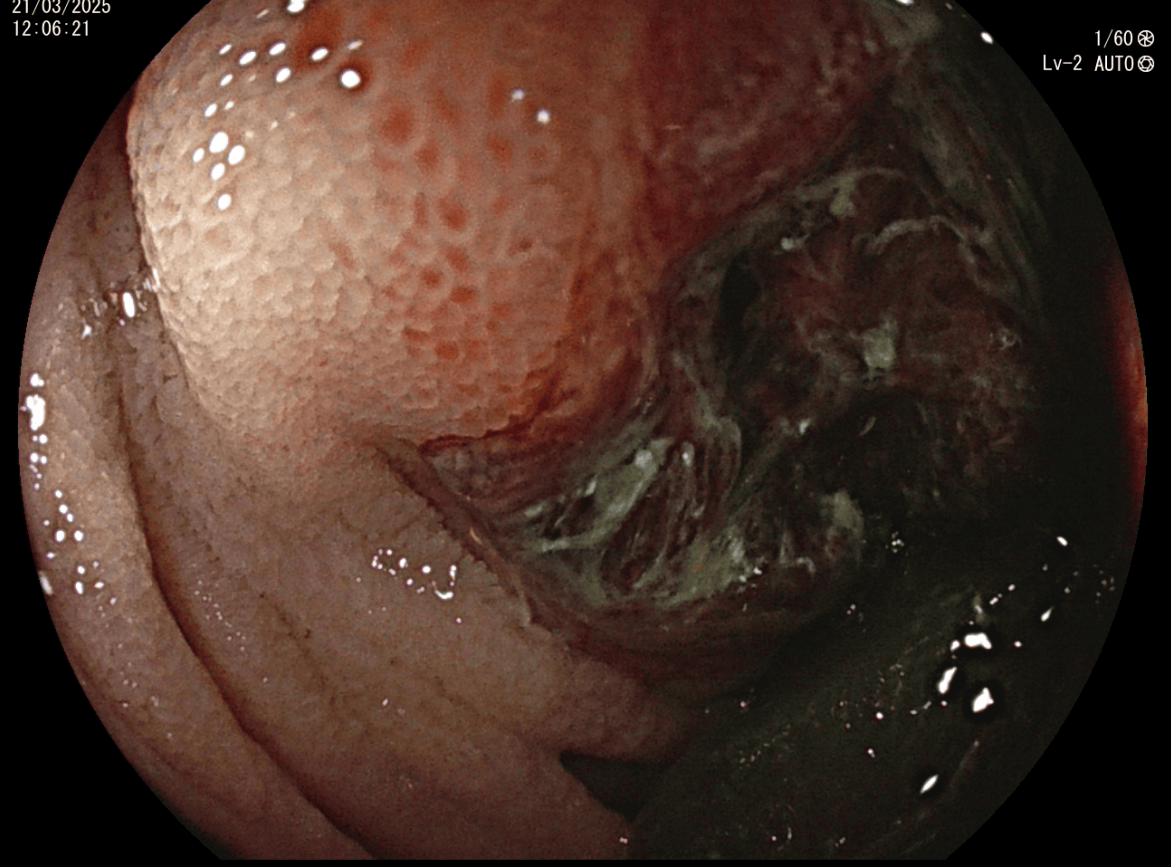
Figure: Biopsy-confirmed metastatic jejunal angiosarcoma on small bowel enteroscopy
Figure: Biopsy-confirmed metastatic jejunal angiosarcoma on small bowel enteroscopy
Disclosures: Christopher Miquel-Chambers indicated no relevant financial relationships. Christiana Shaw indicated no relevant financial relationships. Tiffany Chua indicated no relevant financial relationships.
Christopher A. Miquel-Chambers, MD1, Christiana M. Shaw, MD, MS1, Tiffany Chua, MD2. P1944 - Rare Metastatic Angiosarcoma to the Jejunum in a Patient With a History of Neck Angiosarcoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.