The Wright Center for Graduate Medical Education Scranton, PA
Ali Osman Avci, MD1, Seyma Bayram, MD2, Mostafa Eysha, MD3, Mehmet Talha Bayram, MD4, Mehmet Bektas, MD5 1Lokman Hekim University Ankara Hospital, Ankara, Ankara, Turkey; 2The Wright Center for Graduate Medical Education, Scranton, PA; 3Texas Tech University Health Science Center El Paso, El Paso, TX; 4Geisinger Wyoming Valley Medical Center, Wilkes-Barre, PA; 5Bayindir Private Hospital, Ankara, Ankara, Turkey Introduction: Multiple Myeloma (MM) predominantly involves bone marrow, but extramedullary disease can affect various organs. Gastrointestinal (GI) tract involvement (pancreas, duodenum) is uncommon, presenting significant diagnostic and therapeutic challenges. Manifestations range from incidental surveillance findings to symptoms mimicking primary GI neoplasms or inflammation. Accurate diagnosis via advanced endoscopy like Endoscopic Ultrasound (EUS) with Fine-Needle Aspiration (FNA) is crucial to differentiate MM involvement from other pathologies and guide appropriate MM-directed therapy, considering different prognoses.
Case Description/
Methods: Case 1 (Pancreatic Involvement): A 77-year-old male with known MM and prior cervical spine stabilization was found on routine follow-up imaging to have a 7.5 × 4.5 cm solid, iso- to hypoechoic lesion in the pancreatic body/tail, with perigastric lymphadenopathy. Serum CA 19-9 was normal. EUS revealed a 35 × 60 mm solid lesion with poorly defined borders and iso-hypoechoic echotexture, without pancreatic ductal dilatation. EUS-FNA was pursued for diagnosis.
Case 2 (Duodenal Involvement): A 60-year-old female with diabetes, hyperlipidemia, and MM (post-ASCT) presented with reflux, bloating, epigastric pain, weight loss, and nausea. Nine months prior, EGD for these symptoms showed duodenal polyps, confirmed as plasma cell infiltration (extramedullary MM); she received chemotherapy. Due to polyp growth on surveillance, repeat EGD and EUS were performed. EGD identified multiple 3 cm polypoid lesions in the duodenum's second portion, broad-based with central ulceration. EUS staged these as uT2N0, showing invasion into the muscularis propria, precluding endoscopic resection. Discussion: This series highlights varied presentations and diagnostic considerations of GI involvement in MM. Case 1 showed an incidental pancreatic lesion without obstructive signs; Case 2 had symptomatic duodenal progression despite initial chemotherapy. EUS was pivotal for characterization, tissue acquisition (Case 1), or staging/unresectability (Case 2). The non-specific nature of GI manifestations underscores considering extramedullary MM in patients with known MM and new GI lesions. Histopathological confirmation is paramount for management, often systemic chemotherapy, as GI involvement in MM generally has a poor prognosis. These cases emphasize advanced endoscopy and multidisciplinary care for these rare, significant MM complications.
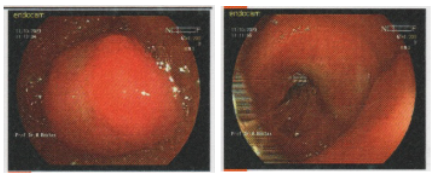
Figure: EGD image showing multiple broad-based polypoid lesions with central ulceration in the second portion of the duodenum.
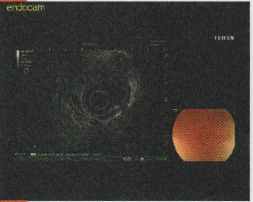
Figure: EUS image demonstrating lesion with invasion into the muscularis propria
Disclosures: Ali Osman Avci indicated no relevant financial relationships. Seyma Bayram indicated no relevant financial relationships. Mostafa Eysha indicated no relevant financial relationships. Mehmet Talha Bayram indicated no relevant financial relationships. Mehmet Bektas indicated no relevant financial relationships.
Ali Osman Avci, MD1, Seyma Bayram, MD2, Mostafa Eysha, MD3, Mehmet Talha Bayram, MD4, Mehmet Bektas, MD5. P1941 - Gastrointestinal Involvement in Multiple Myeloma: A Case Series of Pancreatic and Duodenal Plasmacytomas, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.