Meher Gujral, MBBS1, Astin Worden, MD2, Mashal Batheja, MD3, Kevin Ruff, MD3 1Mayo Clinic, Poughkeepsie, NY; 2Mayo Clinic, Phoenix, AZ; 3Mayo Clinic, Scottsdale, AZ Introduction: Mantle cell lymphoma (MCL) is a type of Non-Hodgkin’s Lymphoma, compromising 7% of all lymphoid neoplasms. It primarily affects older males, presenting with B symptoms, fatigue and lymphadenopathy. Pathogenically, MCL is driven by t(11;14)(q13;32) chromosomal translocation leading to Cyclin D over expression and unchecked B-cell proliferation. While GI involvement is common, primary small bowel MCL presenting as intussusception is exceedingly rare. We report a case of MCL involving the terminal ileum presenting as ileocecal intussusception oncolonoscopy.To our knowledge, only three such cases have been previously described.
Case Description/
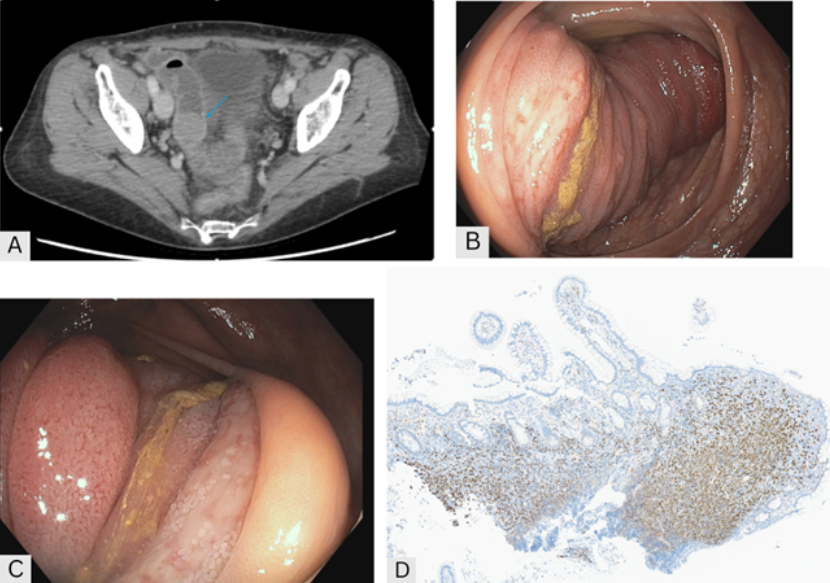
Methods: A 66 year old female with chronic abdominal pain previously felt to be functional in etiology with EGD, colonoscopy, CT enterography, gastric emptying study, and abdominal US 3 years prior largely unrevealing aside from gastric intestinal metaplasia seen on EGD and a subcentimeter gallbladder polyp on US. Surveillance abdominal US showed two calculi in the distal CBD. She underwent elective ERCP with sphincterotomy and cholecystectomy. A year later, she presented with persistent pain, new cramping of the RLQ, and a 15lb unintentional weight loss. A repeat CT abdomen and pelvis with IV contrast revealed an asymmetric mass-like wall thickening of the distal ileum, approximately 20cm from the ileocecal valve (Image A). Balloon-assisted colonoscopy showed distal ileum prolapsing through the ileocecal valve into the cecum (Image B) with nodular and ulcerated mucosa (Image C). Biopsies confirmed MCL, staining positive for cyclin D1 (Image D). Bone marrow biopsy confirmed involvement, but TP53 mutation was negative. She initially chose active surveillance, but PET-CT 1 year later revealed progression, and she was started on R-CHOP chemotherapy. Discussion: This case highlights the need to evaluate GI symptoms particularly when the characteristics change or red flag symptoms like unintentional weight loss develop. GI involvement in MCL is associated with a more aggressive phenotype and can present as Multiple Lymphomatous Polyposis (MLP) or a solitary lesion. However, lesions may be subtle or missed endoscopically. Histologically, MCL features lymphoid cells with irregular nuclear contours and condensed chromatin. Unlike the classic MLP presentation, our case had a mass-like terminal ileal lesion which presented as intussusception- a rare finding in adults, that warrants evaluation for malignancy, including lymphoproliferative disorders.
Figure: A) CT showing asymmetric mass-like wall thickening of the distal ileum measuring 2.8 x 2.6 x 1.2 cm (blue arrow), approximately 20cm from the ileocecal valve B) Balloon-assisted colonoscopy with distal ileum prolapsed into the cecum C) Nodular and ulcerated mucosa of the terminal ileum D) Terminal ileal biopsy staining positive for cyclin D1
Disclosures: Meher Gujral indicated no relevant financial relationships. Astin Worden indicated no relevant financial relationships. Mashal Batheja indicated no relevant financial relationships. Kevin Ruff indicated no relevant financial relationships.
Meher Gujral, MBBS1, Astin Worden, MD2, Mashal Batheja, MD3, Kevin Ruff, MD3. P2025 - More Than a Cramp: Mantle Cell Lymphoma Presenting as Adult Intussusception, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Meher Gujral, MBBS (she/her/hers) photo")