MedStar Georgetown University Hospital Arlington, VA
Samantha Marshall, MD1, Thomas Loughney, MD2 1MedStar Georgetown University Hospital, Arlington, VA; 2MedStar Georgetown University Hospital, Washington, DC Introduction: Bezoars are accumulations of undigested fibrous material in the GI tract that most often occur in the stomach.1Extra-gastric bezoars are rare. We present a case of terminal ileum bezoar in a patient with prior ileocecectomy.
Case Description/
Methods: A 55-year-old male with Crohn’s disease and prior ileocecectomy was referred by surgery for small bowel bezoar. He had undergone ileocecectomy 15 years prior with multiple subsequent small bowel obstructions. Imaging showed a large bezoar in the neoterminal ileum proximal to the anastomosis. He was referred to GI for endoscopic management.
The patient underwent 10 colonoscopies to break apart the bezoar, which initially measured ~6 x 15 cm. Forceps, snares, balloons, and APC were used to fragment the bezoar, but progress was limited by its hard outer shell and mobile nature.
In later procedures, large portions were removed. Days after his tenth colonoscopy, the patient developed rectal pain. Exam revealed a rectal bezoar, which was manually fragmented and removed. He has since remained symptom-free. Discussion: Small bowel bezoars are rare, causing only 4% of all SBO-related hospitalizations.3 This case highlights an unusual presentation of an ileal bezoar in a patient with abnormal anatomy. Bezoars are typically gastric and linked to delayed motility or prior gastric surgery.1 Though colonic and rectal seed-bezoars have been reported, these occur mostly in children or those with high-seed diets.2
This case presents several considerations. The patient’s altered anatomy from ileocecectomy likely predisposed him to bezoar formation, and while bezoars are not common in Crohn's disease, enterolithiasis is a known complication caused by strictures and stasis. It is plausible that narrowing at the anastomosis or unknown proximal strictures contributed to the formation of this patient's bezoar.
Bezoars should be considered in patients with recurrent obstruction and a history of bowel surgery or Crohn’s disease, as timely endoscopic evaluation may offer both diagnosis and effective treatment. References
Bouali S, et al. Phytobezoar: An unusual cause of small bowel obstruction. Ann Med Surg (Lond). 2021;62:323-325. doi: 10.1016/j.amsu.2021.01.048.
Eitan A, et al. Fecal impaction in adults: report of 30 cases of seed bezoars in the rectum. Dis Colon Rectum. 2006;49(11):1768-71. doi: 10.1007/s10350-006-0713-0.
Delabrousse E, et al. Small-Bowel Bezoar Versus Small-Bowel Feces: CT Evaluation. Am J Roentgenol. 2012; 191(5): 1465-1468. doi: 10.2214/AJR.07.4004.
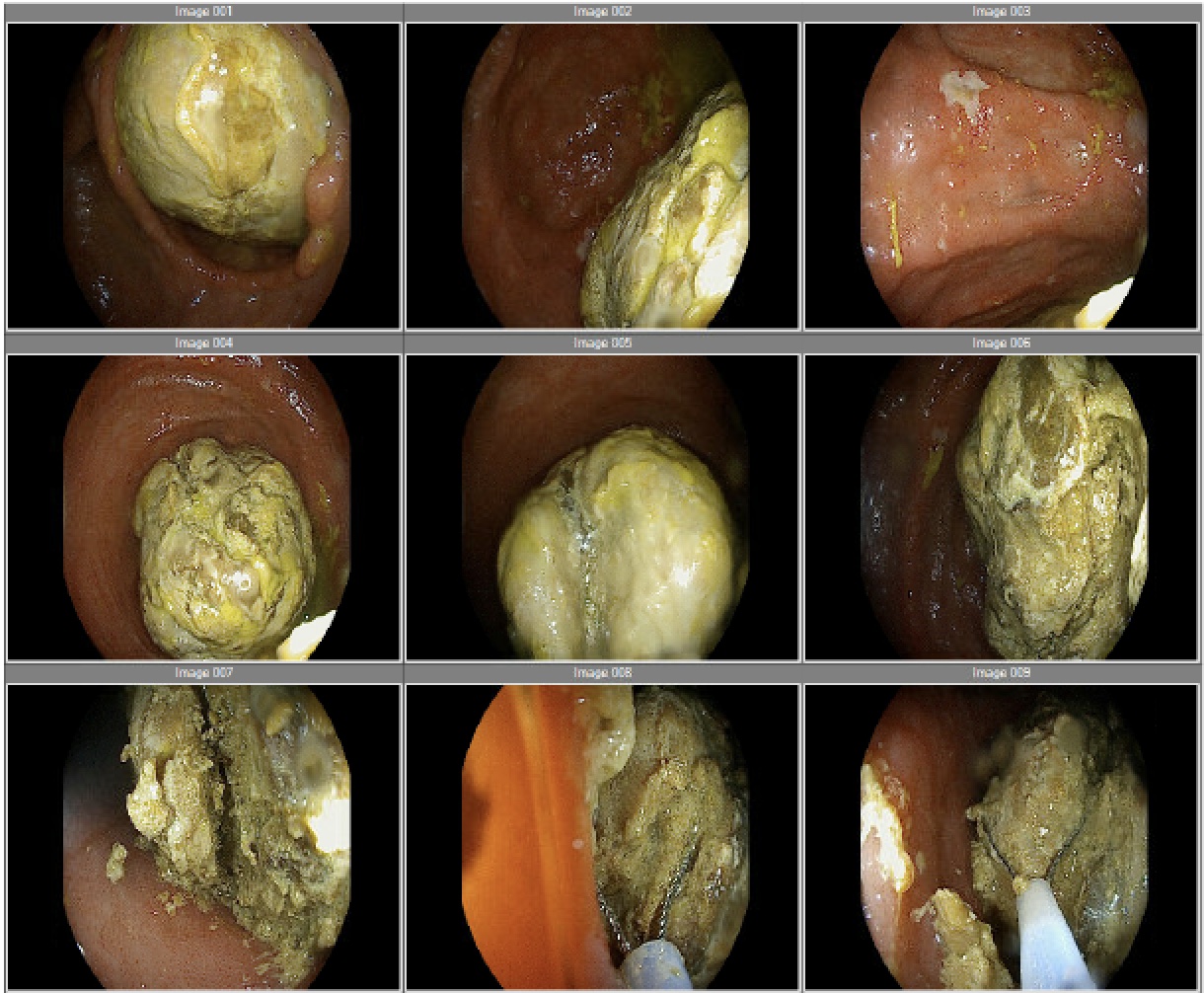
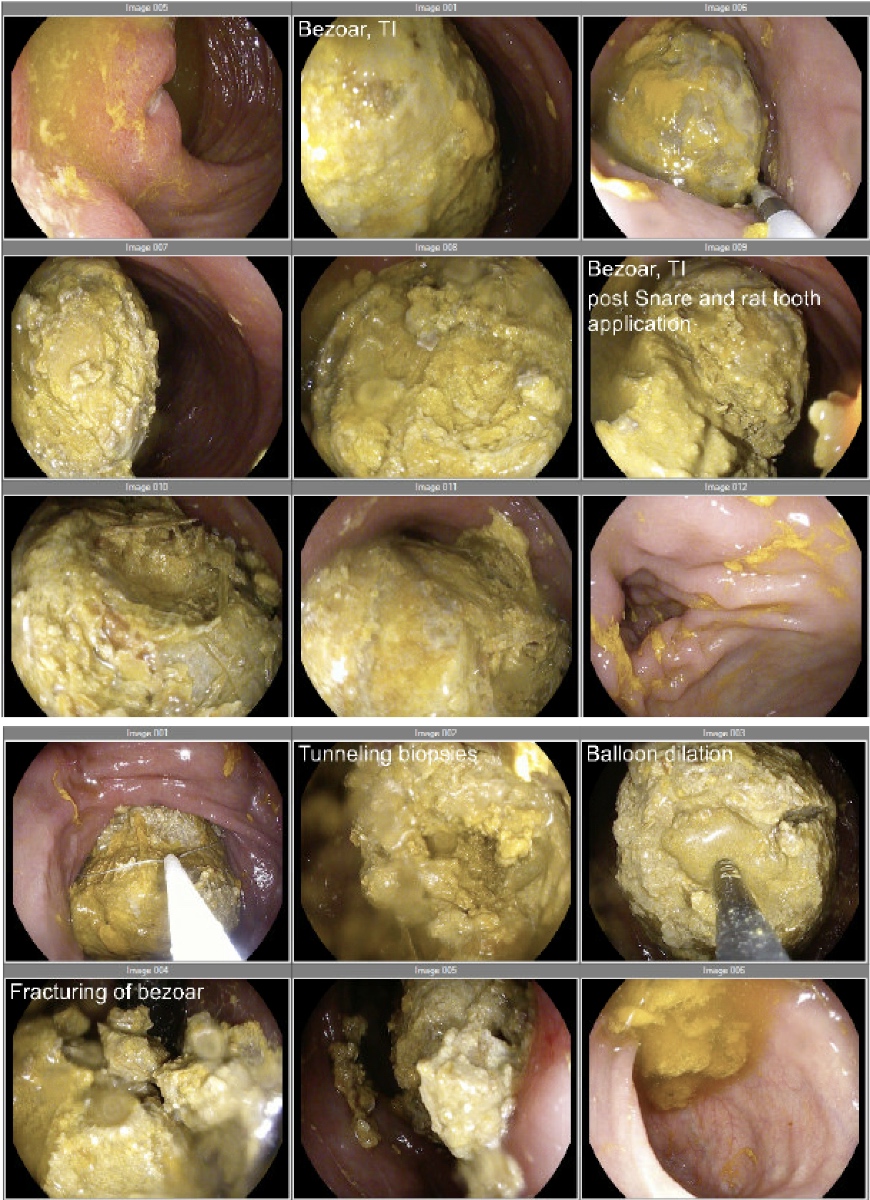
Figure: Figure 1: Initial colonoscopy revealing ~6 x 15 cm bezoar in the neoterminal ileum. Multiple techniques utilized to fragment the bezoar including snare, rat tooth forceps, and balloon dilation.
Figure: Figure 2: Final colonoscopy revealing persistent large bezoar in neoterminal ileum. A combination of ESD knife and snare were used to break off 40% of the bezoar over a total of 3.5 hours.
Disclosures: Samantha Marshall indicated no relevant financial relationships. Thomas Loughney indicated no relevant financial relationships.
Samantha Marshall, MD1, Thomas Loughney, MD2. P2022 - How Bezoar! a Rare Case of Small Bowel Bezoar, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.