Yun-Yee Tsang, DO1, Lorraine Chong Tai, MD1, Monica Paneru, DO1, Andrea Escalante, DO2 1Broward Health Medical Center, Fort Lauderdale, FL; 2Broward Health Medical Center, Miami, FL Introduction: A Hiatal Hernia (HH) is a condition of abnormal protrusion of the stomach through diaphragmatic hiatus. A large HH can have life-threatening complications including volvulus, obstruction, ischemia, pulmonary aspiration, or cardiac compression.
Case Description/
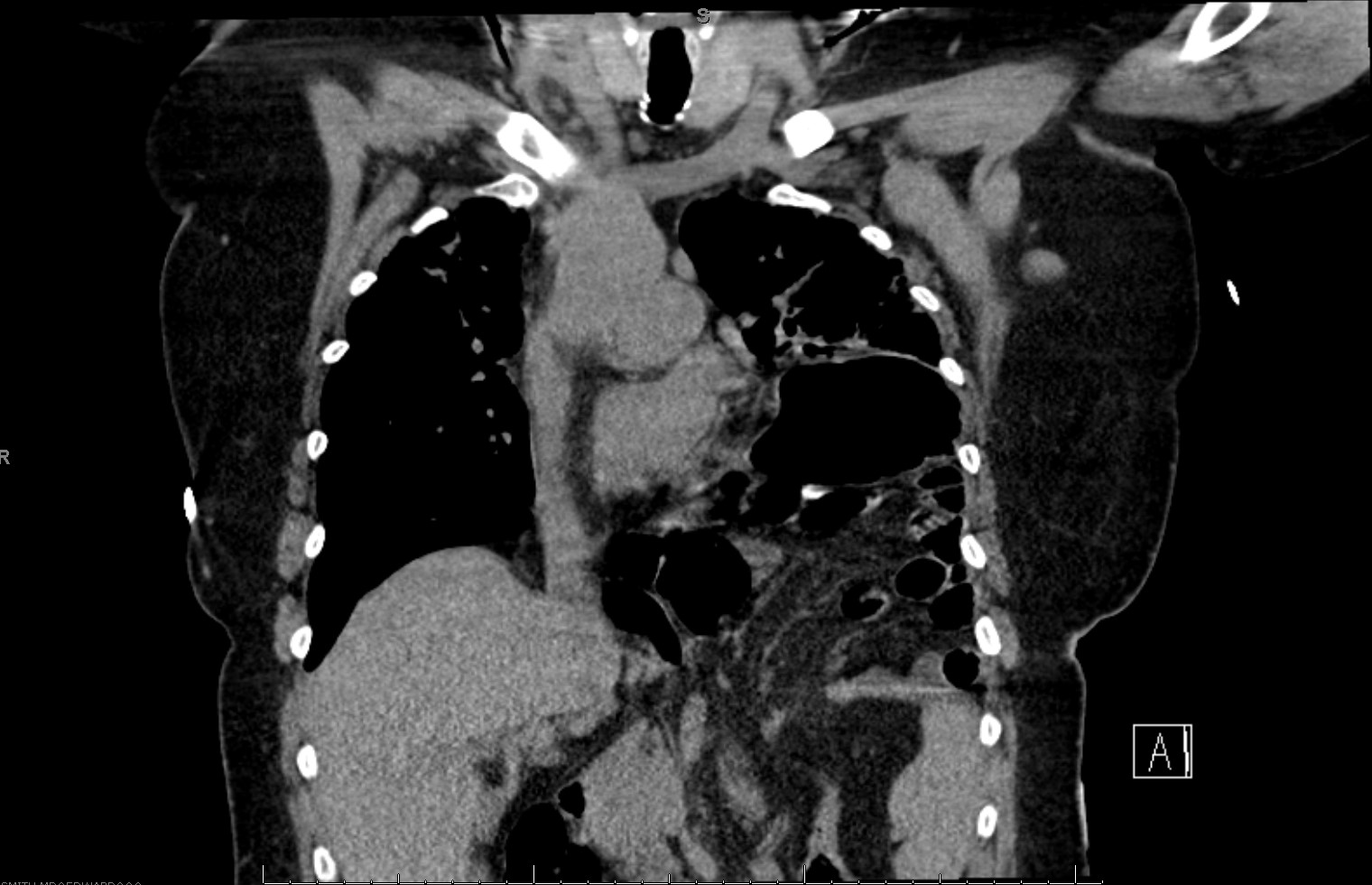
Methods: A 60-year-old female with a history of a paraesophageal hernia and asthma presented for dyspnea and a productive cough for 2 days. She denied any recent travel. A respiratory viral panel was unremarkable and Computed Tomography (CT) Chest confirmed bilateral pneumonia with a large hiatal hernia, with the stomach protruding into the left chest (Figure 1). She was initially started on steroids, bronchodilators, Azithromycin and Ceftriaxone, however her respiratory requirements continued to increase, requiring Bilevel Positive Airway Pressure (BiPAP) and later intubation. Further imaging revealed worsening of severe bilateral ground glass and consolidative airspace opacities. Sputum cultures grew Rothia mulcinaginosa and antibiotics were switched to piperacillin-tazobactam. The patient’s oxygenation failed to improve with proning trials and was placed on Veno-venous Extracorporeal membrane oxygenation (V-V ECMO). She later developed cholecystitis, bacteremia, fungemia and progressed to renal failure. Due to poor prognosis, the family withdrew care. Discussion: Given the large size of this hernia, the absence of any viral infection or recent travel, we highly suspected her pneumonia was secondary to silent aspiration. Current guidelines indicate surgical repair for symptomatic paraesophageal hernias, particularly in cases of obstruction or volvulus and shared decision making for asymptomatic patients. Elective surgery may be considered for
asymptomatic paraesophageal hernias, however this approach remains controversial. There is currently insufficient data to adequately compare the benefits and risks of conservative management against elective surgery for asymptomatic cases. There is limited data regarding the hiatal hernias progression and subsequent complications. Our patient was diagnosed with a
paraesophageal hernia in 2017 and remained asymptomatic until presentation. Surgical repair was offered, but the patient declined. There is currently limited research comparing conservative management to prophylactic surgical repair for asymptomatic paraesophageal hernias. This case emphasizes the need for clearer clinical guidelines to inform the management of asymptomatic paraesophageal hernias and prevent catastrophic outcomes.
Figure: Figure 1: Coronal view of CT Chest showing large hiatal hernia with stomach in left chest
Disclosures: Yun-Yee Tsang: Enzolytics – Stocks that have been sold. Lorraine Chong Tai indicated no relevant financial relationships. Monica Paneru indicated no relevant financial relationships. Andrea Escalante indicated no relevant financial relationships.
Yun-Yee Tsang, DO1, Lorraine Chong Tai, MD1, Monica Paneru, DO1, Andrea Escalante, DO2. P2091 - Atypical Presentation of Large Hiatal Hernia Triggering Aspiration Pneumonia and Acute Respiratory Distress Syndrome (ARDS), ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.