Palak Patel-Rodrigues, DO1, Sumair Ahmad, MD2 1Henry Ford Hospital, Detroit, MI; 2Henry Ford Health, Detroit, MI Introduction: Organoaxial malrotation of the stomach is historically observed in the setting of a gastric volvulus. In this event, the stomach is rotated along its long axis placing the gastric antrum and pylorus in an anterior position when compared to the gastroesophageal junction. However, this anatomical presentation of the stomach is rarely observed without a gastric volvulus. We describe a case presentation of non-volvulus gastric organoaxial malrotation likely secondary to a prior complicated gastric band surgery.
Case Description/
Methods: A 45 year old male with a past medical history of gastric band surgery complicated by iatrogenic esophageal perforation with surgical repair in 2008 status post lap-band removal presented to clinic for months of epigastric pain and intermittent nausea unrelated oral intake. He did not endorse any dysphagia or regurgitation symptoms. Prior to this, he had presented to the emergency room with severe abdominal pain. He was found to have normal labs including liver enzymes and a CT abdomen/pelvis which revealed no evidence of acute cholecystitis, however, it did show gallstones. He was discharged with famotidine with moderate improvement He denied a prior upper endoscopy or colonoscopy. He underwent upper endoscopy (EGD) that showed a regular Z-line as well as evidence of a prior gastric band as characterized by a sharp and acute angulation of the gastric antrum, pre-pyloric segment, and pylorus. He was then recommended to obtain an upper gastrointestinal (GI) series to evaluate his anatomy given the observed "V-shaped/J-shaped" stomach. This study showed an organoaxial malrotation of the stomach without a volvulus. Discussion: For our patient, the organoaxial malrotation of his stomach as evidenced on his EGD and upper GI series waslikely secondary to a previous complicated lap-band placement and removal years ago. His imaging did not show evidence of a gastric volvulus. Typically when this anatomy is observed it is in the setting of a gastric volvulus. This case highlights the importance of considering this condition when patients present with typical dyspepsia symptoms and a history of prior gastric band surgery. In the case of this patient, his symptoms improved moderately with conservative measures such as dietary changes and a H2 blocker, however, if symptoms are severe and non-responsive to medications, endoscopic or surgical intervention to detorse the stomach can be offered.
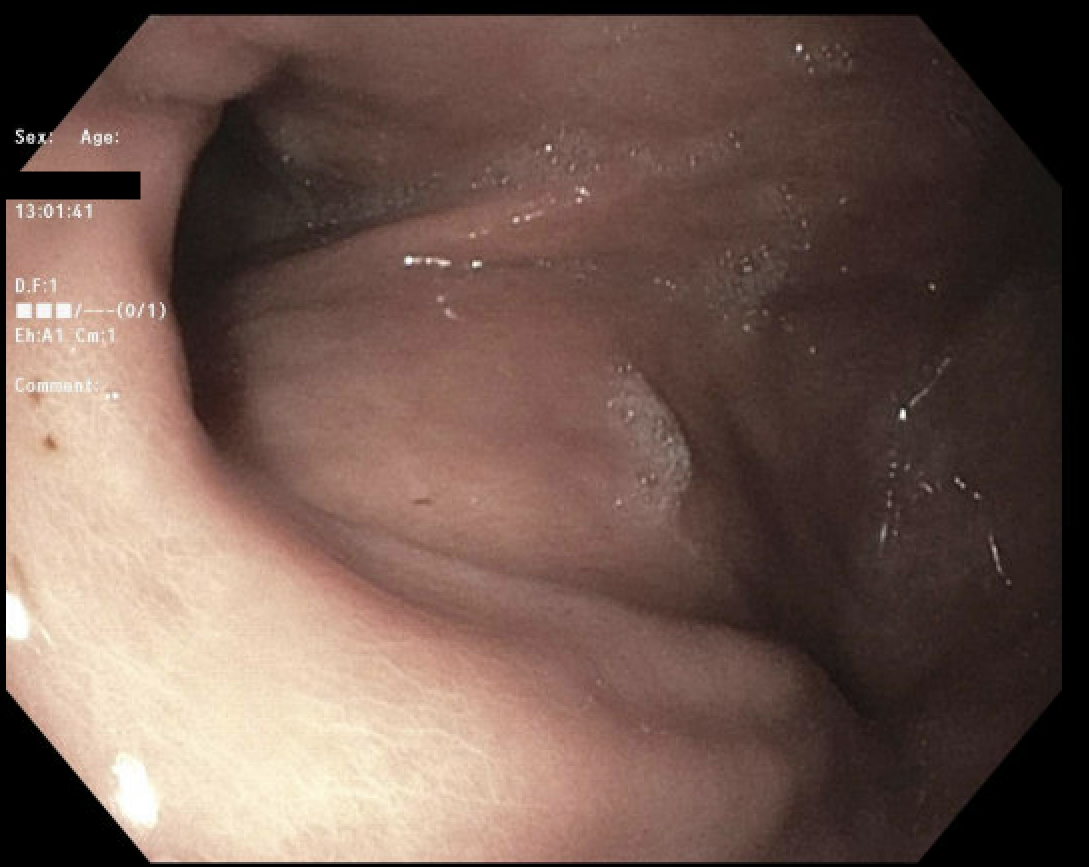
Figure: Evidence of sharp angulation of the gastric antrum, pre-pyloric segment, and pylorus on upper endoscopy
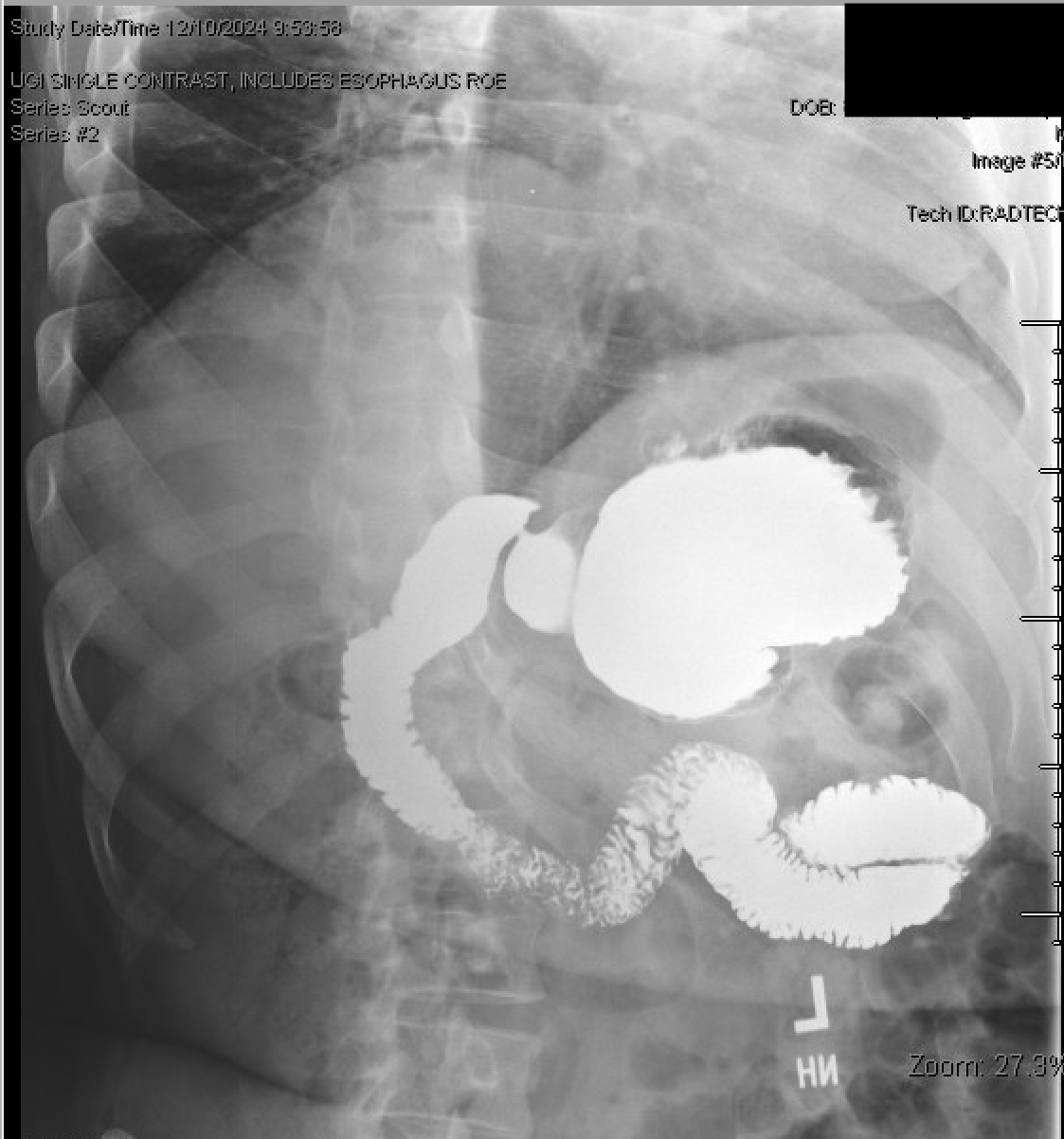
Figure: Organoaxial malrotation of the stomach without volvulus as seen on upper gastrointestinal series
Disclosures: Palak Patel-Rodrigues indicated no relevant financial relationships. Sumair Ahmad indicated no relevant financial relationships.
Palak Patel-Rodrigues, DO1, Sumair Ahmad, MD2. P2088 - A Rare Case of Non-Volvulus Gastric Organoaxial Malrotation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.