Aditya Vyas, MD1, Rohit Goyal, MD2, Karan Sachdeva, MD3, Hassaan Zia, MD4, Kshitij Arora, MD3, Sarav Daid, MD5, Qiang Cai, MD, PhD, MACG6 1LSUHS, Shreveport, LA; 2Louisiana State University, Shreveport, LA; 3LSU Health, Shreveport, LA; 4Medical College of Wisconsin, Milwaukee, WI; 5LSU Health Shreveport, Shreveport, LA; 6LSU Health Sciences Center - SHREVEPORT, LA, Shreveport, LA Introduction: Sarcoidosis is a chronic,non-caseating granulomatous systemic inflammatory disease.It can involve any organ,most commonly the lungs.GI involvement is rare and may present either as part of systemic disease or as an isolated finding.We present an interesting case of gastric sarcoidosis in a female presenting with epigastric pain and reflux symptoms.
Case Description/
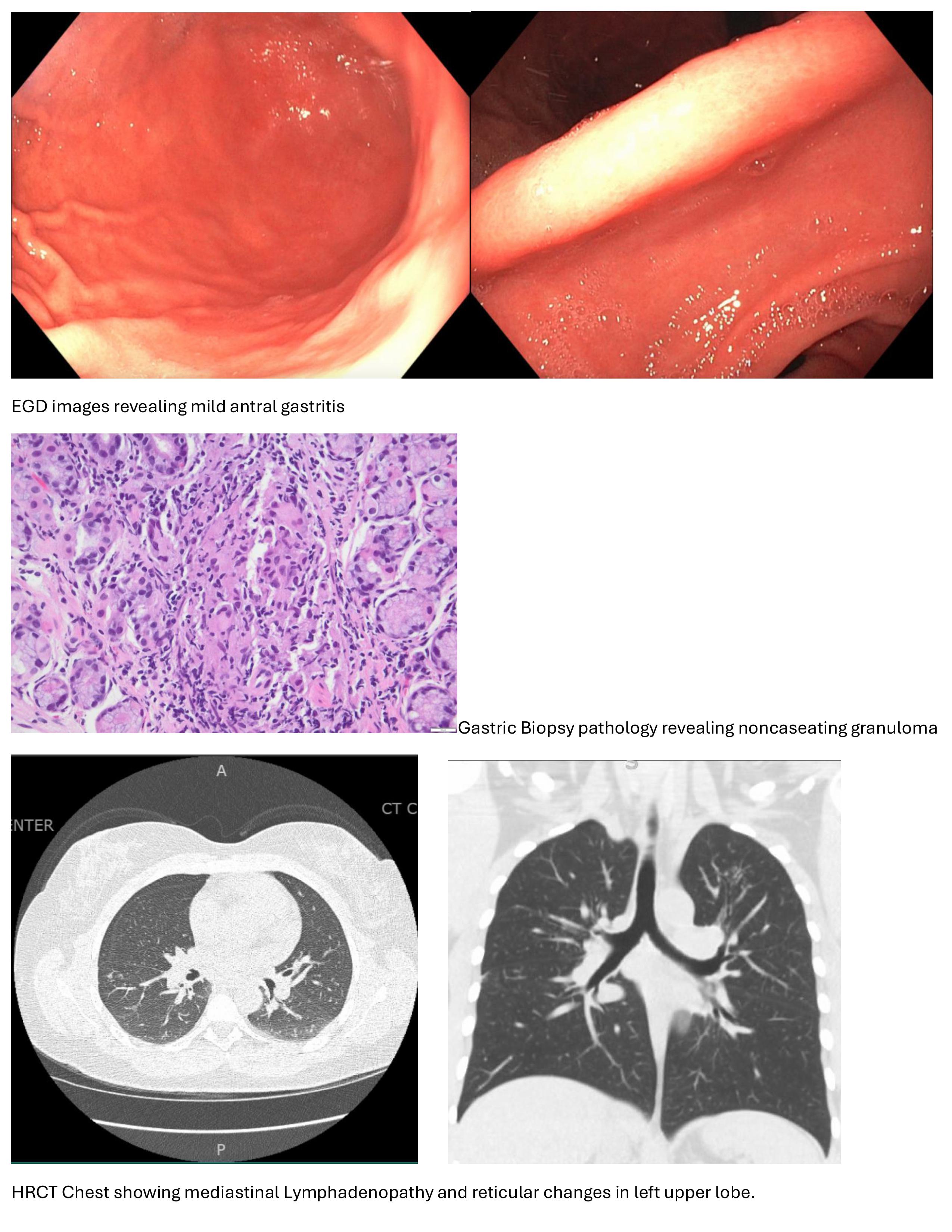
Methods: A 36-year-old African American female with no significant past medical history presented to the family medicine clinic with a 4-month history of a chronic,dry cough.She reported no associated fever or weight loss.Her social history was notable for an 8-year history of chronic cigarette use.She denied any recent travel or family history of similar symptoms.In addition to her cough,the patient complained of persistent epigastric pain unrelated to food intake,along with reflux symptoms unresponsive to PPI therapy.Initial workup with a CBC and CMP was unremarkable except for mild anemia (hgb 11.4 g/dL) and low iron saturation (9%).A CXR and PFT were unremarkable.Due to persistent GI symptoms and anemia,the patient was referred to gastroenterology.EGD revealed a normal esophagus, antral gastritis, and a normal duodenum.Gastric biopsies were obtained.Histopathology of the gastric biopsy revealed noncaseating granulomas,raising suspicion for sarcoidosis,particularly in the context of her chronic cough.The patient was referred to pulmonology and rheumatology for further evaluation. An HRCT scan of the chest revealed mediastinal lymphadenopathy and reticular changes in the left upper lobe.Further lab testing showed an elevated ACE level of 118 U/L,an ESR of 35 mm/hr,CRP of 4.5 mg/L.The patient was started on a short course of corticosteroids and initiated on mycophenolate mofetil.After 2 months of therapy,the patient reported significant improvement in both her cough and epigastric pain.Mild reflux symptoms persisted but were well controlled with ongoing PPI therapy. Discussion: Gastric sarcoidosis is a rare manifestation that can mimic other GI conditions.Its diagnosis requires careful evaluation,as noncaseating granulomas may also be seen in several other conditions.The differential diagnosis includes PUD,Ménétrier disease,hypertrophic gastritis,infections such as Mycobacterium or Histoplasma,syphilis,gastric malignancies,lymphoma,Langerhans cell histiocytosis,foreign body reactions,Crohn’s disease,and Whipple’s disease.Accurate diagnosis is important,as treatment strategies vary significantly depending on the underlying etiology.
Figure: Images from Endoscopy, pathology slides and HRCT scan of the chest
Disclosures: Aditya Vyas indicated no relevant financial relationships. Rohit Goyal indicated no relevant financial relationships. Karan Sachdeva indicated no relevant financial relationships. Hassaan Zia indicated no relevant financial relationships. Kshitij Arora indicated no relevant financial relationships. Sarav Daid indicated no relevant financial relationships. Qiang Cai indicated no relevant financial relationships.