Vaishnavi K. Modi, MD1, Mahader N. Wossene, MD2, Anum Nawaz, MBBS, MD1, Rekik A. Degef, MD2, Zohaib Haque, DO3, Yanping Wang, MD, PhD4 1MacNeal Hospital Loyola Medicine, Oak Park, IL; 2MacNeal Hospital Loyola Medicine, Berwyn, IL; 3MacNeal Hospital Loyola Medicine, Chicago, IL; 4Loyola University Medical Center, Maywood, IL Introduction: Cholangiocarcinoma (CCA) is a rare malignancy originating from the biliary epithelium, accounting for ~3% of gastrointestinal (GI) and ~15% of primary liver cancers. It predominantly affects males in their 60s to 70s and is associated with risk factors such as primary sclerosing cholangitis (PSC), chronic biliary inflammation, cirrhosis, and liver fluke infections, particularly in Southeast Asia. CCA often presents with nonspecific symptoms such as jaundice, weight loss, and abdominal pain. However, pleural effusion as an initial manifestation is exceedingly rare. We present a unique case of intrahepatic CCA presenting with recurrent pleural effusions.
Case Description/
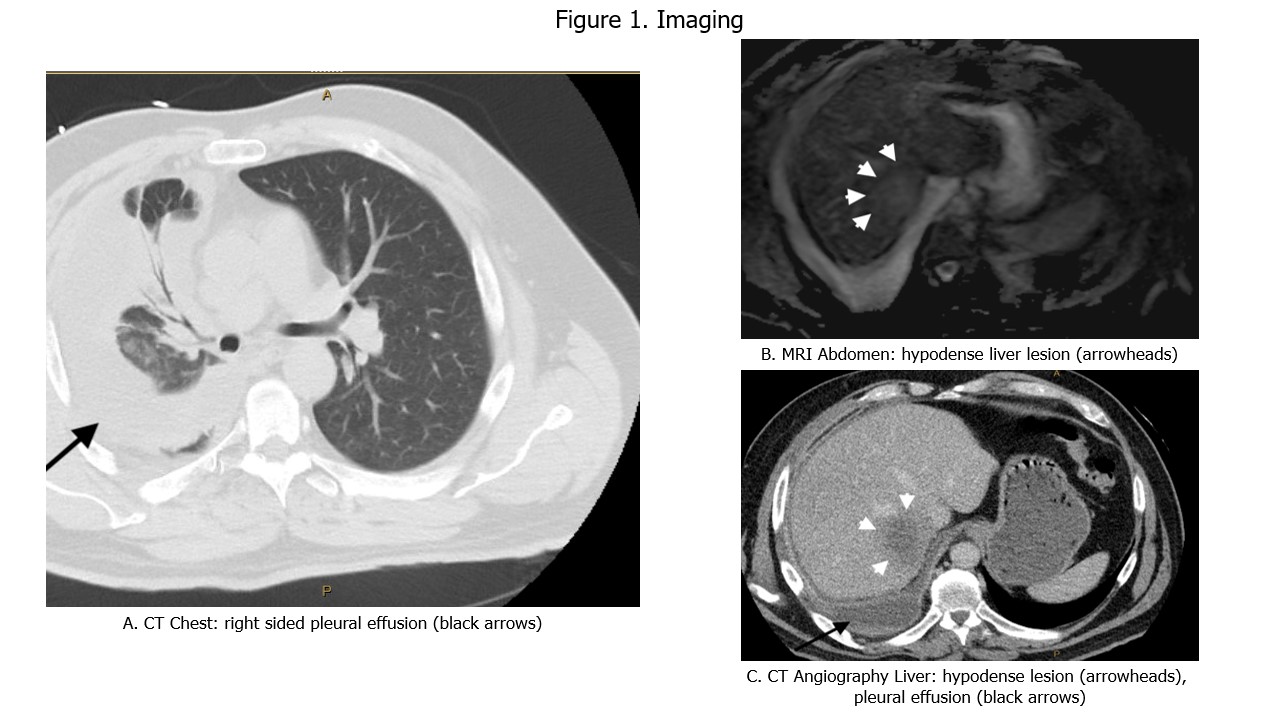
Methods: A 61-year-old Middle Eastern male with no significant medical history presented with progressive dyspnea and pleuritic chest pain. Chest imaging revealed a new right-sided pleural effusion (Figure 1A). Diagnostic thoracentesis yielded exudative fluid with elevated WBC counts; cytology was negative for malignancy. Empiric antibiotic therapy provided mild symptomatic relief.
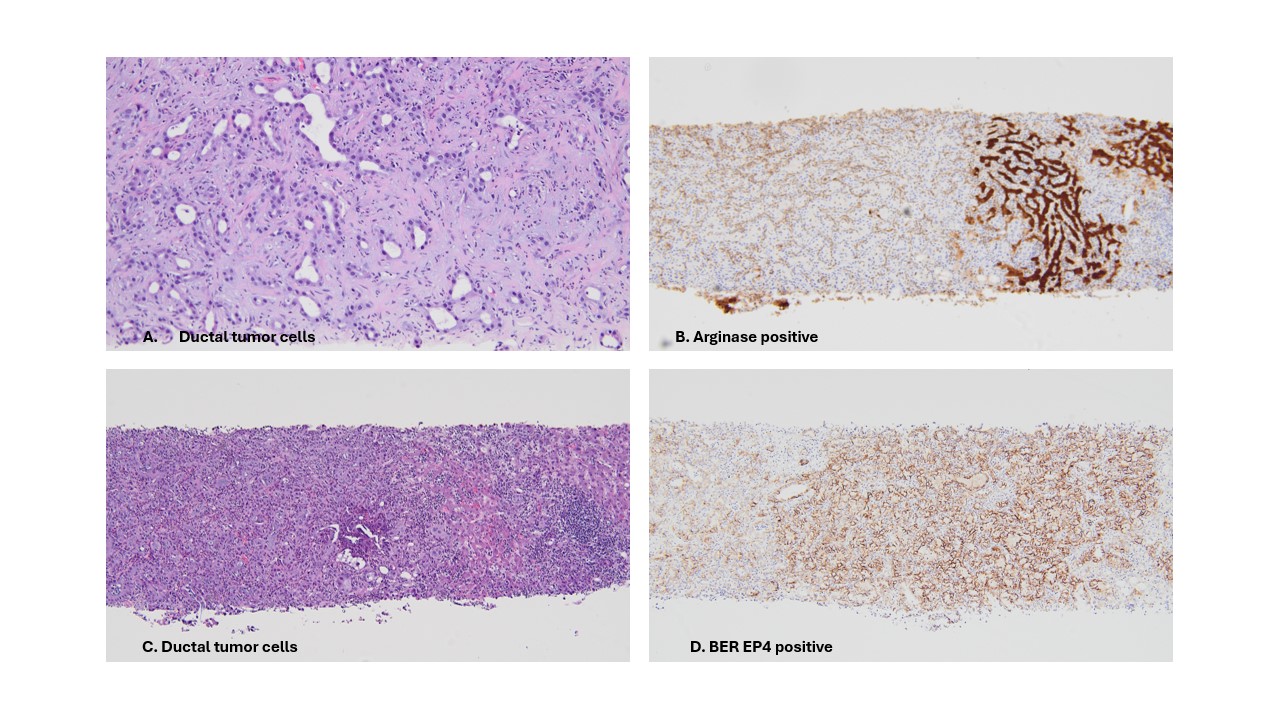
The patient returned within days with recurrent symptoms. Repeat imaging demonstrated a persistent right-sided pleural effusion and an incidental hypodense lesion in the liver (Figure 1B, 1C). Laboratory studies showed normal liver function tests, alpha-fetoprotein (AFP), and carcinoembryonic antigen levels; however, CA 19-9 was elevated. Initial liver biopsy was nondiagnostic. Due to high clinical suspicion, a second biopsy was performed, revealing malignant epithelial cells (Figure 2A, 2C). Immunohistochemical staining was positive for Ber-EP4 and MOC31 (Figure 2D), markers indicative of pancreaticobiliary origin, confirming the diagnosis of intrahepatic cholangiocarcinoma. Patient elected for hospice care. Discussion: Our case highlights a rare and diagnostically challenging presentation of intrahepatic cholangiocarcinoma (CCA) initially manifesting as recurrent pleural effusions. Most CCA-related pleural effusions are malignant and occur later in the disease. In contrast, our patient's effusion was the initial clue. Negative pleural cytology does not exclude malignancy. Elevated CA 19-9 may raise suspicion, but definitive diagnosis relies on histopathology. Given biopsy sensitivities as low as 60–70%, repeat sampling is often necessary. Early recognition of atypical presentations is crucial, as CCA has a poor prognosis with a median survival of 12–24 months. This case adds to the limited literature.
Figure: Figure 1. Pleural effusion and liver lesion imaging
Figure: Figure 2. Biopsy images
Disclosures: Vaishnavi Modi indicated no relevant financial relationships. Mahader Wossene indicated no relevant financial relationships. Anum Nawaz indicated no relevant financial relationships. Rekik Degef indicated no relevant financial relationships. Zohaib Haque indicated no relevant financial relationships. Yanping Wang indicated no relevant financial relationships.
Vaishnavi K. Modi, MD1, Mahader N. Wossene, MD2, Anum Nawaz, MBBS, MD1, Rekik A. Degef, MD2, Zohaib Haque, DO3, Yanping Wang, MD, PhD4. P2385 - A Diagnostic Detour: When Pleural Effusion Leads to Cholangiocarcinoma Diagnosis!, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")