University of Alabama at Birmingham Hospital Birmingham, AL
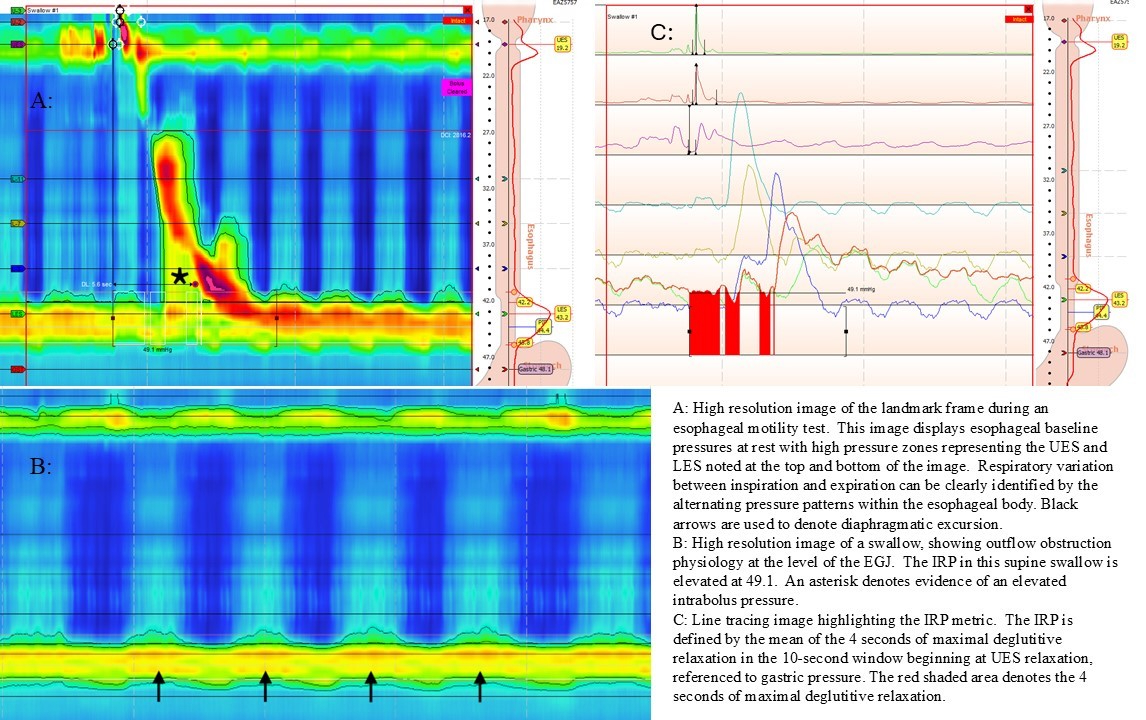
Charles D.. Evers, MD, MBA1, Hayden Shuster, MD, PharmD1, John Cooper, MD2, James Callaway, MD3 1University of Alabama at Birmingham Hospital, Birmingham, AL; 2University of Alabama at Birmingham Heersink School of Medicine, Birmingham, AL; 3Basil I. Hirschowitz Endoscopic Center of Excellence, The University of Alabama at Birmingham Heersink School of Medicine, Birmingham, AL Introduction: Esophageal manometry (HRM) is used to evaluate esophageal pressure during deglutition. Esophagogastric junction (EGJ) relaxation is measured by the IRP on HRM. EGJ outflow obstruction (EGJOO) is a heterogeneous physiologic condition with both mechanical and non-mechanical etiologies. EGJOO is a motility disorder defined by an elevated IRP, >20% of swallows with evidence of elevated intrabolus pressure, and the presence of esophageal peristalsis. Increased diaphragmatic pressure during inspiration applies pressure to the EGJ (Figure 1). We hypothesized that tachypnea, defined as respiratory rate (RR) ≥20, may lead to artifactual increases in supine and upright IRP and an artifactual diagnosis of EGJOO. Methods: In 2023, 69 patients completed HRM as part of lung transplant evaluation. Patient demographics, indication for lung transplant, and HRM data were recorded by retrospective chart review. RR was calculated by reviewing HRM tracings during the landmark frame.
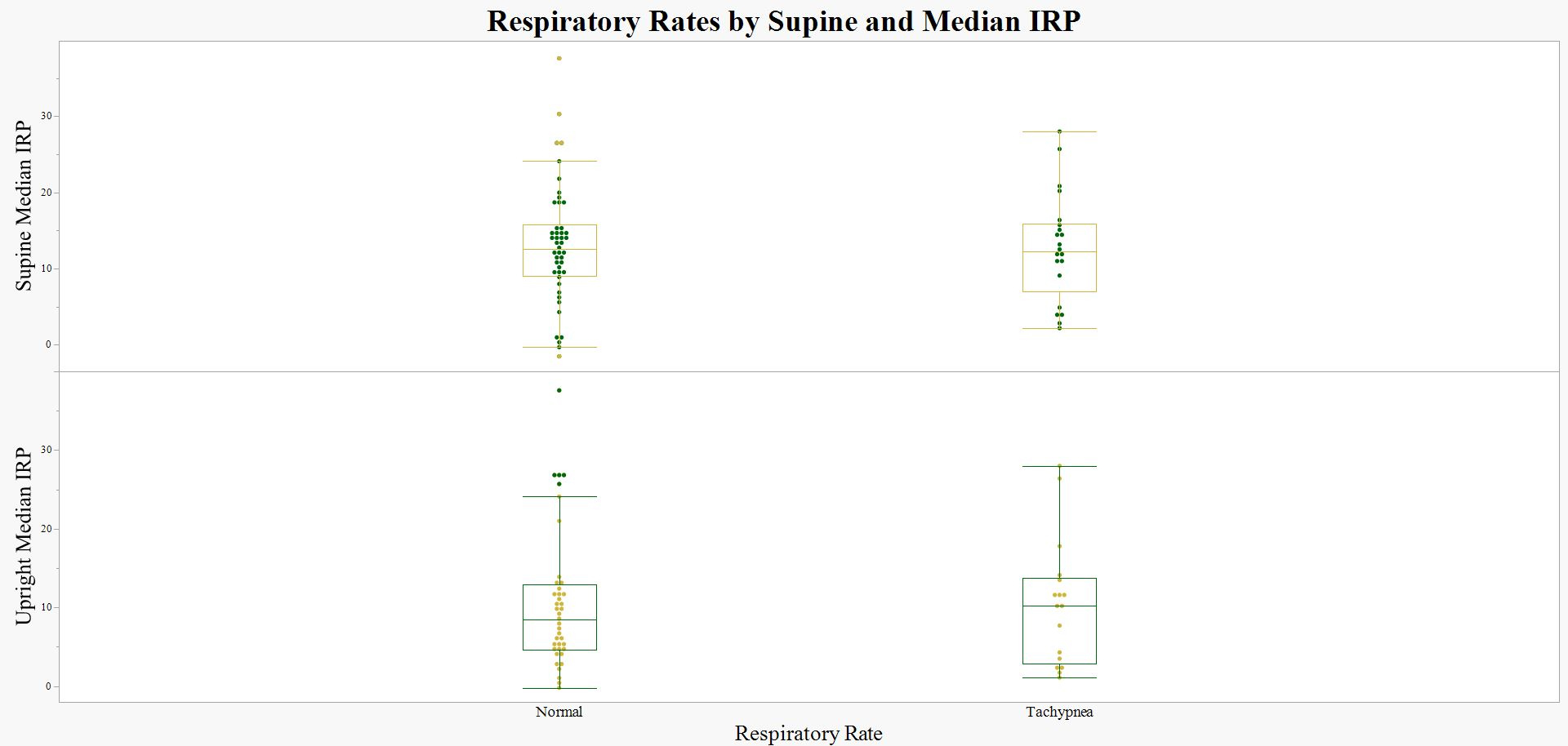
Data analyses were performed using JMP® 18 software. The distributions of the supine and upright IRP values were analyzed for normality using q-q plots and histogram visual inspection. As the IRP values were not equally distributed and our sample size with EGJOO was small, nonparametric tests were utilized. Supine and upright IRP were compared to respiratory rates utilizing the Wilcoxon Rank Sum Test. Results: The median supine IRP in those without EGJOO was 12, and with EGJOO was 27.5 (p=0.0012). The median upright IRP in those without EGJOO was 9.2, and with EGJOO was 28.7 (p = 0.0014). In those with normal RR, median supine IRP was 12.99 and those with tachypnea was 12.77 (p = 0.4436). In those with normal RR, the median upright IRP was 10.56, and for those with tachypnea, it was 10.45 (p = 0.4205, Figure 2). Discussion: Esophageal dysmotility is common in patients undergoing evaluation for lung transplantation. In this study, tachypnea is not associated with an elevated IRP, and thus a diagnosis of EGJOO. This validates the use of IRP to diagnose outflow obstruction disorders in patients with tachypnea. If EGJOO is found on esophageal motility testing, additional testing should be pursued, including the currently recommended confirmatory testing which may include a timed barium esophagram or EndoFLIP. The study may be limited by sample size (n: 69).
Figure: Figure 1
Figure: Figure 2: Comparison of respiratory rates measured in supine position and median integrated relaxation pressure (IRP) during high-resolution manometry, illustrating the relationship between body position and esophageal motility metrics
Disclosures: Charles Evers indicated no relevant financial relationships. Hayden Shuster indicated no relevant financial relationships. John Cooper indicated no relevant financial relationships. James Callaway indicated no relevant financial relationships.
Charles D.. Evers, MD, MBA1, Hayden Shuster, MD, PharmD1, John Cooper, MD2, James Callaway, MD3. P2772 - Breath Easy: Tachypnea Is Not Associated With an Elevated Integrated Relaxation Pressure (IRP) in Lung Transplant Candidates, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.