Rutgers Robert Wood Johnson University Hospital North Brunswick, NJ
James D. Lee, MD1, Michael Ma, MD2, Arvind Trindade, MD2, Petros Benias, MD2 1Rutgers Robert Wood Johnson University Hospital, North Brunswick, NJ; 2Rutgers Robert Wood Johnson University Hospital, New Brunswick, NJ Introduction: Surgically alteredgastrointestinal anatomy is becoming more common as surgical interventions are employed for conditions such as congenital anomalies, cancer resection, and bariatric surgery. These anatomies pose a challenge for endoscopic retrograde cholangiopancreatography (ERCP), often precluding the use of standard duodenoscopy equipment. As many alternative approaches such as intervention endoscopic ultrasound arise, balloon-assisted ERCP should strongly be considered for tackling such anatomical variants. However, balloon-assisted ERCP is often limited by availability of accessory devices due to their long and narrow working channel.
Case Description/
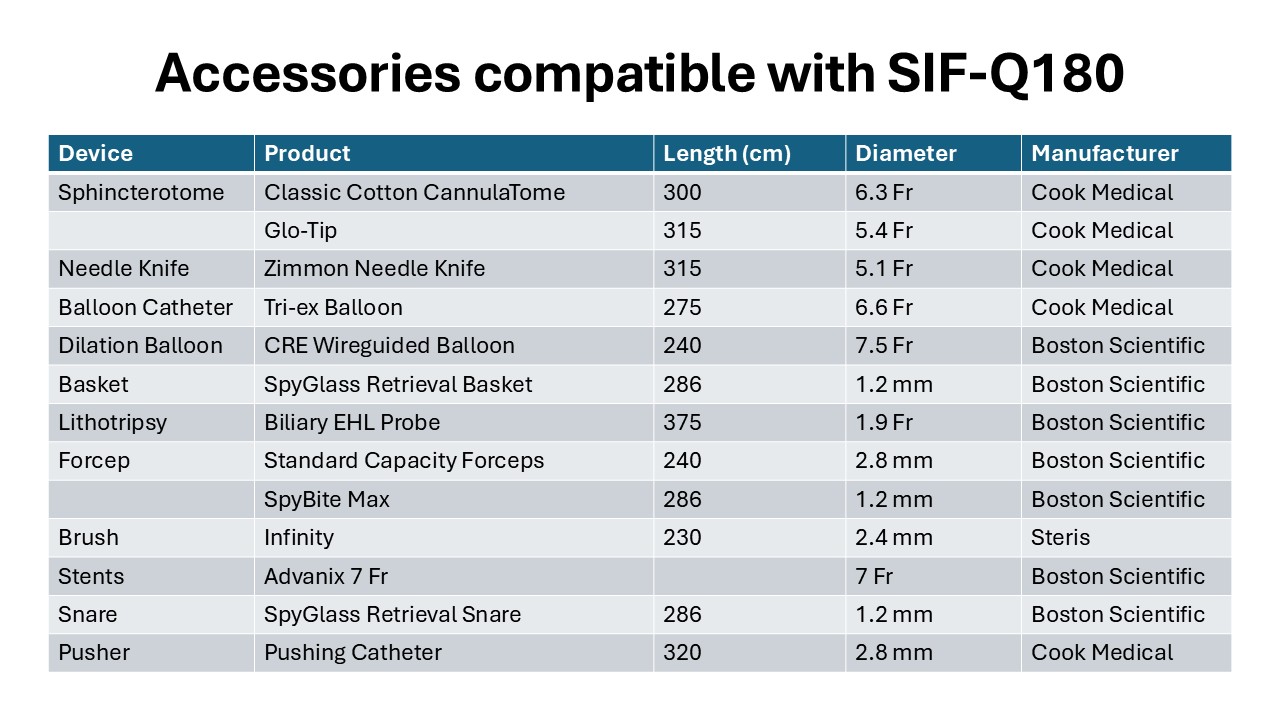
Methods: A 71-years-old female with history of Whipple’s procedure for pancreatic cancerinitially presented with a severe pinhole hepaticojejunostomy (HJ) stricture on initial ERCPwhich was treated with dilation and stent placement. She returned for balloon-assisted ERCP with SIF-Q180 (Video 1). The previous stent was removed, and intraoperative cholangiogram demonstrated a filling defect at the distal bile duct consistent with choledocholithiasis. Following dilation of the HJ stricture, standard balloon extraction was attempted unsuccessfully. Next, stone extraction using a cholangioscopic retrieval basket was attempted.The basket was deployed proximally to the stone followed by back and forward motion to capture the stone within the basket. After capture, the basket was closed to secure the stone and surrounding debris before removal. The culprit stone was successfully extracted, and three stents were placed at the HJ stricturefor remodeling. Discussion: Balloon-assisted ERCP is an essential procedure for the rapidly growing population with altered anatomy requiring ERCP, and thus it is crucial that accessory devices compatible with the dimensions of ERCP scopes are developed. This case presents anapplication of a cholangioscopy retrieval basket in balloon-assisted ERCP (Figure 1).The length and diameter of the selected duodenoscope allowed for smoother deployment in areas with limited stability and alternative endoscopic approach.
Figure: Accessories compatible with SIF-Q180
Disclosures: James Lee indicated no relevant financial relationships. Michael Ma indicated no relevant financial relationships. Arvind Trindade: Exact Sciences – Consultant, Grant/Research Support. Lucid Diagnostics – Consultant, Grant/Research Support. Petros Benias: Aurora Medical Technologies – CMO, Co-Founder. Boston Scientific – Consultant. Micro-tech Endoscopy – Consultant.
James D. Lee, MD1, Michael Ma, MD2, Arvind Trindade, MD2, Petros Benias, MD2. P2731 - Harnessing Single-Balloon ERCP to Address Biliary Pathology in Patients With Altered Anatomy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")