Andrej M. Sodoma, DO1, Brendan Ryu, MD2, Mark Baginski, DO2, Mary Thomas, DO2, Antonio Costantino, MD2 1Northwell Health, Lake Grove, NY; 2Northwell Health, Bay Shore, NY Introduction: Iliopsoas abscess (IPA) is a rare infection in the iliopsoas muscle. They often present with non-specific symptoms, leading to diagnostic delays. In this case report, we discuss a rare incidence of iliopsoas abscess due to a fistula from the sigmoid colon caused by the patient's complex history of cancer, chemotherapy, and radiation treatment, which was closed by an endoscopic clip.
Case Description/
Methods: A patient in her 80s presented to the hospital with frequent watery diarrhea, vomiting, and abdominal pain after undergoing chemotherapy with Irinotecan three weeks before the day of admission. She had a history of metastatic urethral cancer to the liver with neuroendocrine features, cystectomy with urostomy, lumbar compression fracture, and anemia of chronic disease. The patient was started on Zosyn 3.375 IVPB every 12 hrs due to unstable Cr for empiric coverage. CT of the abdomen and pelvis showed a large left iliopsoas abscess measuring at least 7 x 4 x 11 cm and a fistula between the abscess and the adjacent sigmoid colon. Colorectal surgery was consulted; the patient was deemed a poor surgical candidate. Interventional radiology (IR) was consulted, and a 12F drain was placed into the left psoas collection with drainage of pus/stool. The cultures of the iliopsoas abscess resulted in various bacteria and yeast, likely stool. Blood cultures had no growth. After deeming the patient a poor surgical candidate for abscess removal/debridement and fistula removal/closure, the patient was left with no source control. Advanced endoscopy was consulted. The patient was deemed a suitable candidate for fistula closure via endoscopy. The patient underwent a colonoscopy; the fistula was visualized, and argon plasma coagulation (APC) and three hemostatic clips were used to close the fistula. IR removed the drain. The patient was discharged to home hospice. Discussion: Endoscopic modalities of gastrointestinal (GI) fistula closure include stents clips, sutures, tissue sealants, endoscopic vacuum, and cardiac septal occluders. In colonic fistula, closure of the etiologies of malignancy, Crohn’s, or post-surgical using stents has a success rate of 50–70%. However, the success rate for hemostatic clips is unknown as they are not routinely used. Hemostatic clips have advantages: they are easier to use, less technical, and less likely to migrate than stents. However, they are restricted to minor defects of 2–3 cm diameter. In this case, three hemostatic clips were used with successful fistula closure.
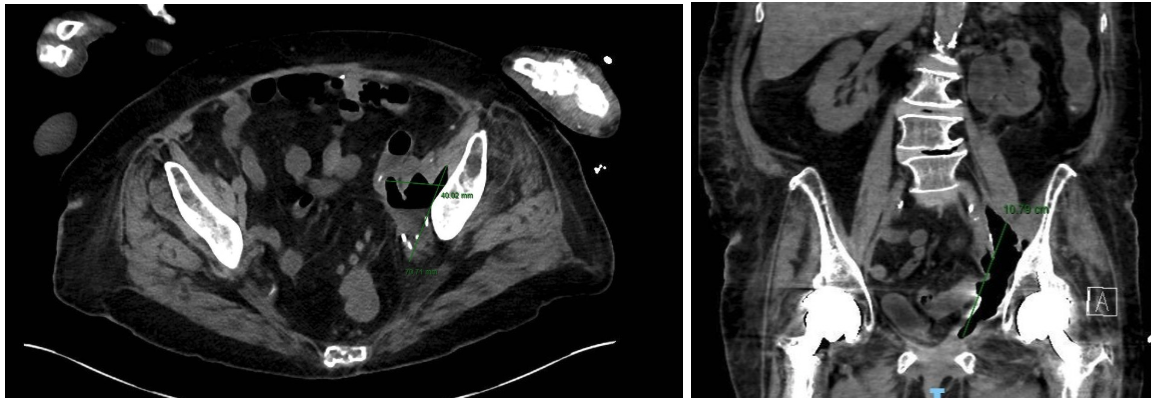
Figure: CT 1 day after admission showed no signs of intrabdominal or retroperitoneal bleed, a 7x4 cm left iliopsoas abscess with fluid and gas, and a fistula to the adjacent sigmoid colon.
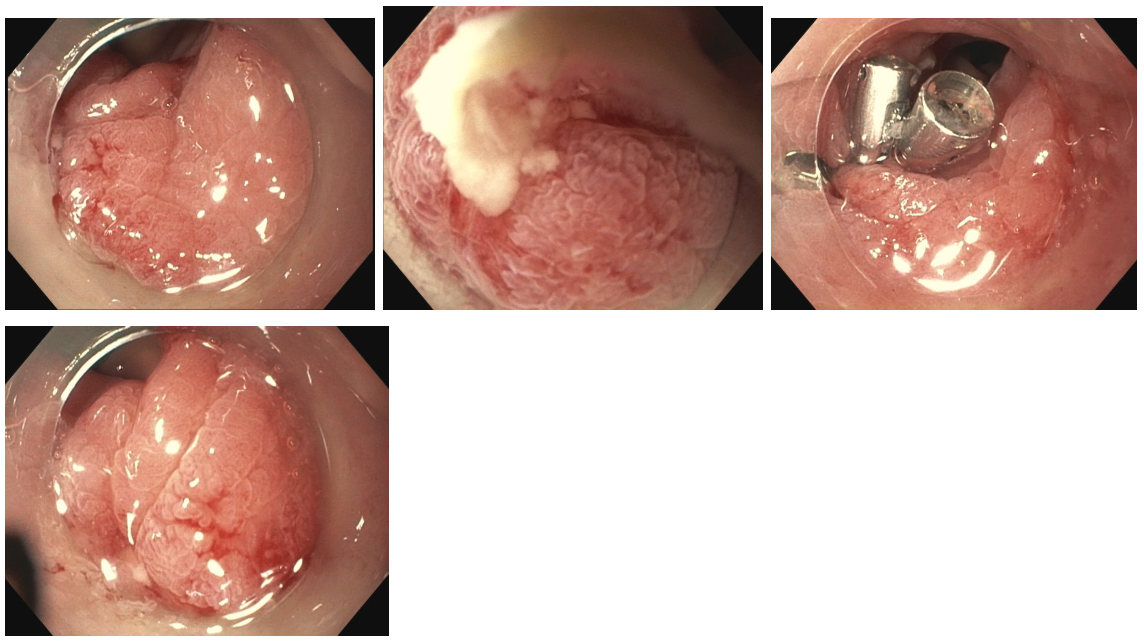
Figure: Endoscopic images demonstrate white pustular exudate coming from the opening of the fistula. Then, the placement of 3 hemostatic clips.
Disclosures: Andrej Sodoma indicated no relevant financial relationships. Brendan Ryu indicated no relevant financial relationships. Mark Baginski indicated no relevant financial relationships. Mary Thomas indicated no relevant financial relationships. Antonio Costantino indicated no relevant financial relationships.
Andrej M. Sodoma, DO1, Brendan Ryu, MD2, Mark Baginski, DO2, Mary Thomas, DO2, Antonio Costantino, MD2. P2526 - Closure of a Fistula Connecting the Sigmoid Colon to the Iliopsoas Abscess Through Endoscopic Clip, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.