
Monday Poster Session
Category: Colon
 photo")
Riddhi Machchhar, DO (she/her/hers)
Hackensack Meridian OUMC
Brick, NJ
IP remains an enigmatic condition in clinical practice, with no clear consensus on its etiology. While often incidental, the diagnosis requires careful differentiation from more common causes of free air in the abdomen, emphasizing the importance of thorough evaluation and management
Case Description/
Methods:
A 76 yo F w/ PMHx DM II, HLD, medullary thyroid cancer post-thyroidectomy, CHF presented to the ER after her Holter monitor revealed intermittent 3rd degree AVB. She was asymptomatic with no complaints. On presentation, she was stable, with normal vitals except for occasional dips in HR to the 40s. A CXR revealed pneumomediastinum, prompting further imaging. A CT scan showed not only pneumomediastinum but also pneumoperitoneum in the upper abdomen, raising concern for a possible perforated viscus.
She was admitted to the ICU for monitoring with placement of a temporary TVP pending PPM placement. Despite the concerning imaging, her clinical exam showed a soft, non-tender abdomen with no signs of acute distress, and her lab work remained stable.
Gen surg performed a diagnostic ex-lap, which revealed no perforation, though the presence of sevoflurane in the abdomen suggested an abnormal communication between the thorax and abdomen, potentially from a ruptured mediastinal bleb. The ex-lap ruled out a perforated viscus or colon.
A PPM was successfully placed, and the patient was discharged in stable condition on oral AC, with plans for close follow-up and monitoring.
Discussion: Idiopathic pneumoperitoneum (IP) is a rare subtype of pneumoperitoneum, and a diagnosis of exclusion. It typically requires conservative management and serial monitoring. It is most often caused by GI perforation, with other manifestations like pneumatosis intestinalis and portal venous gas linked to acute GI ischemia, both associated w/ high mortality rates. Theories on the pathogenesis of IP include mechanical pressure, bacterial gas production, and intra-mural gas blebs, the latter of which was considered in this case as a potential cause for free air in the peritoneum. IP can be found incidentally in asymptomatic patients, often during routine screenings such as CXRs or CT scans. These patients may not exhibit typical signs of peritonitis, making diagnosis particularly challenging. Management of IP is typically conservative, with careful observation. Although recurrence is rare, there have been instances of IP reappearing years later, necessitating long-term monitoring.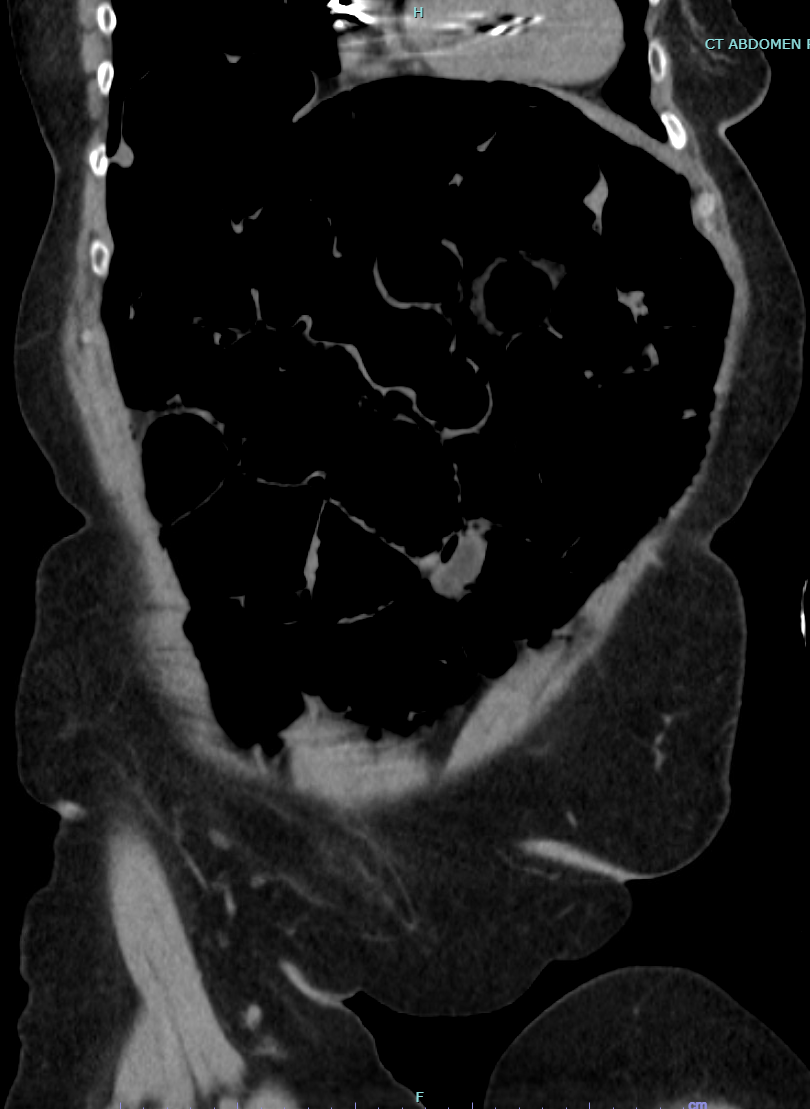
Figure: CT Abdomen/Pelvis without contrast - pneumomediastinum and pneumoperitoneum, concerning possible colonic perforation, though no clear area of perforation noted on imaging
Disclosures:
Riddhi Machchhar indicated no relevant financial relationships.
Matthew Friedland indicated no relevant financial relationships.
Eric Ball indicated no relevant financial relationships.
Emad Kamel indicated no relevant financial relationships.
Stephen Klepner indicated no relevant financial relationships.
Riddhi Machchhar, DO, Matthew Friedland, MD, Eric Ball, MD, Emad Kamel, MD, Stephen Klepner, DO. P2497 - Incidental, Idiopathic Pneumoperitoneum in an Asymptomatic Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.