
Monday Poster Session
Category: Colon

Yesol Oh, MD
Wright State University
Dayton, OH
The risk of colorectal cancer (CRC) is increased in patients with a history of diverticulitis. However, undiagnosed CRC can coexist with diverticulitis, complicating its presentation and diagnosis. We report a case of a 57-year-old female who presented with symptoms of diverticulitis refractory to antibiotics and was later found to have an obstructing sigmoid mass, which was revealed to be stage IIIb sigmoid adenocarcinoma.
Case Description/
Methods:
A 57-year-old female with a past medical history of stage IV chronic kidney disease, iron deficiency anemia and gastroesophageal reflux disease presented with left lower quadrant pain, chills, and constipation. A non-contrast computed tomography (CT) scan of the abdomen and pelvis revealed acute diverticulitis of the sigmoid colon with a pericolonic mass concerning for an abscess (Figure 1). The abscess was initially deemed too small for IR-guided drainage, and the patient was admitted for diverticulitis and started on intravenous piperacillin-tazobactam. Despite appropriate antibiotic therapy, the patient’s constipation persisted, prompting a repeat CT scan with rectal contrast. Imaging results were consistent with persistent bowel obstruction, though it was unclear if the etiology was of inflammatory or malignant origin. The patient underwent flexible sigmoidoscopy, which revealed a mechanical obstruction with adhesion of sigmoid colon to anterior abdominal wall. During the procedure, the colon was separated from the abdominal wall, revealing the known abscess which was suctioned. A firm mass in the distal sigmoid colon, approximately 40 cm from anal verge, was also identified (Figure 2). The patient subsequently underwent robot-assisted sigmoid colectomy with end colostomy. The procedure was uneventful, and the obstruction was resolved. Pathology from the resected specimen confirmed stage IIIb adenocarcinoma of the sigmoid colon. The patient was discharged in stable condition with plans for outpatient oncology follow-up.
Discussion:
This case highlights the importance of considering malignancy in patients with atypical presentations of diverticulitis, especially with persistent symptoms and no prior documented screening for colorectal cancer, as in the case of this patient. It also highlights limitations of cross-sectional CT imaging in identifying undiagnosed colorectal masses. In our case, early surgical intervention not only addressed acute bowel obstruction, but also enabled prompt oncological evaluation and treatment planning.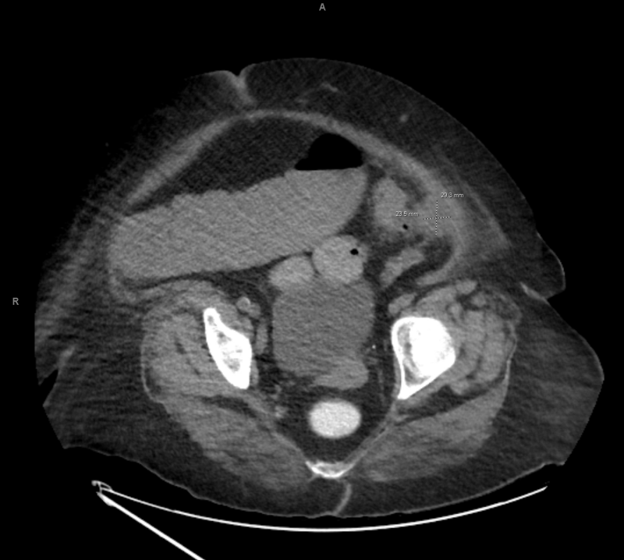
Figure: Figure 1: Axial view of a non-contrast CT of the abdomen and pelvis demonstrates scattered sigmoid diverticula with adjacent fat stranding consistent with diverticulitis. There is a superimposed soft tissue mass measuring 2.9 by 2.4 cm.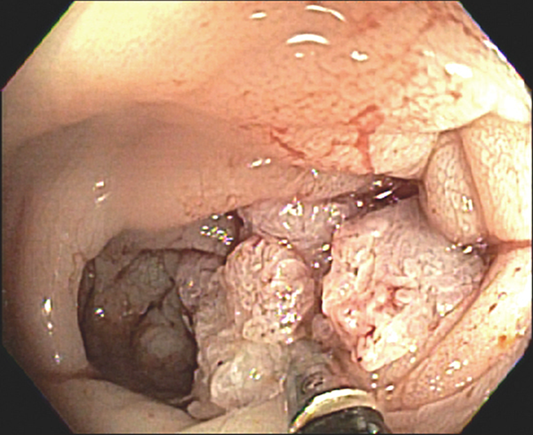
Figure: Figure 2: Flexible sigmoidoscopy shows a firm mass in the distal sigmoid colon, approximately 40 cm from anal verge
Disclosures:
William Jevnikar indicated no relevant financial relationships.
Urmimala Chaudhuri indicated no relevant financial relationships.
Yesol Oh indicated no relevant financial relationships.
Zachary Simmons indicated no relevant financial relationships.
William Jevnikar, MS1, Urmimala Chaudhuri, DO2, Yesol Oh, MD1, Zachary Simmons, MD1. P2473 - Unmasking Colonic Adenocarcinoma: A Case of Sigmoid Diverticulitis With Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.