Hansani Angammana, MD, Judith Berger, MD St. Barnabas Hospital, Bronx, NY Introduction: Burkholderia cepacia is a gram-negative opportunistic pathogen known for its association with pulmonary infections in cystic fibrosis and immunocompromised patients. It is multidrug-resistant and thrives in moist environments, including hospital settings. While bloodstream infections with B. cepacia are rare, they have been linked to contaminated medical equipment. This case is unique as B. cepacia is not typically associated with pancreatitis or cholecystitis, highlighting the need for broad differential diagnoses in complex intra-abdominal infections.
Case Description/
Methods: A 40-year-old male with a history of hypertension, hyperlipidemia, and Roux-en-Y gastric bypass (RYGB) presented with acute epigastric pain, nausea, and vomiting. Labs revealed leukocytosis (WBC 20,600), elevated lipase (1,829), and acute kidney injury (creatinine 1.8). Imaging confirmed acute pancreatitis, gallstones, and a dilated common bile duct (CBD). He was started on IV fluids, ceftriaxone, and metronidazole for suspected biliary infection.
On hospital Day 3, he developed a fever (102.2°F), prompting repeat blood cultures and escalation to meropenem. Despite broad-spectrum antibiotics, he continued to have fevers and was admitted to the intensive care unit (ICU) due to worsening respiratory status and fluid overload. Repeat imaging showed pancreatic necrosis and a phlegmon. Laparoscopic cholecystectomy revealed chronic cholecystitis. Blood cultures grew B. cepacia, resistant to meropenem but sensitive to ceftazidime and levofloxacin. Meropenem was discontinued, and the patient improved on ceftazidime and metronidazole. By Day 7, he was transitioned to oral levofloxacin and metronidazole for three weeks and discharged in stable condition.
The patient was readmitted with recurrent abdominal pain, and imaging revealed a large pancreatic cyst. Endoscopic ultrasound (EUS)-guided cystogastrostomy with necrosectomy was performed, successfully clearing the pseudocyst cavity. Discussion: B. cepacia is an exceptionally rare cause of infection in pancreatitis and pancreatic necrosis. Unlike common intra-abdominal pathogens, its presence in this setting is unusual and suggests possible hospital-acquired transmission. Its biofilm formation and intrinsic antibiotic resistance complicate treatment, requiring targeted therapy. This case highlights the importance of considering atypical pathogens in complex intra-abdominal infections and the role of susceptibility-guided therapy in managing resistant organisms.
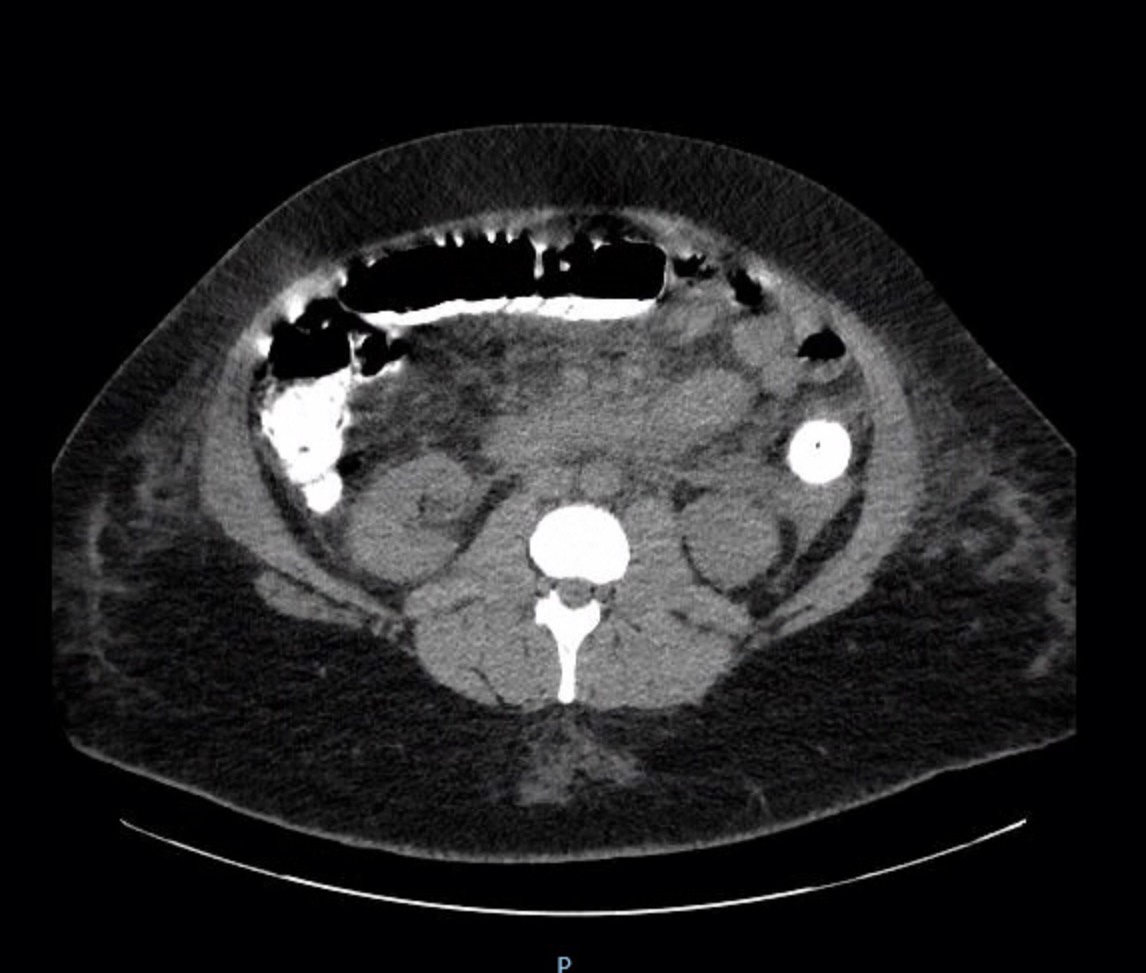
Figure: CT scan on admission showing pancreatitis with phlegm
Figure: CT on the second admission showed a large pancreatic pseudocyst
Disclosures: Hansani Angammana indicated no relevant financial relationships. Judith Berger indicated no relevant financial relationships.
Hansani Angammana, MD, Judith Berger, MD. P2351 - A Rare Case of <i>Burkholderia Cepacia</i> Sepsis in the Setting of Severe Gallstone Pancreatitis and Pancreatic Necrosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.