Philip Hall, MD, MPH1, Vikash R. Chadive, MBBS2, Harman Sawhney, DO3, Taofeek Kolade, MD1, Ayesha Samad, MD4, Fatima Safi. Arslan, MD1, Arsalan Ahmad, MD1, Shreyas Kunjir, MD5, Karim Akl, MD6 1CarePoint Health - Bayonne Medical Center, Bayonne, NJ; 2Bayonne Medical Center, North Bergen, NJ; 3CarePoint Health - Bayonne Medical Center, Melville, NY; 4Ocean University Medical Center, Brick, NJ; 5St. George's University School of Medicine, Belmont, MA; 6Jersey City Medical Center, Jersey City, NJ Introduction: Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin’s lymphoma, presenting as a rapidly growing mass in older adults. It can occur in nodal or extranodal regions, with primary pancreatic lymphoma being a rare but important differential diagnosis for pancreatic head masses. Symptoms are often non-specific and include abdominal pain, weight loss, and jaundice. Distinguishing pancreatic lymphoma from adenocarcinoma is crucial, as treatment and prognosis differ significantly. Notably, necrosis in DLBCL can worsen prognosis and reduce treatment response.
Case Description/
Methods: A 74-year-old female with hypertension, hypothyroidism, and Crohn’s disease presented for an endoscopic ultrasound (EUS) after a low-dose CT scan revealed a 6 cm pancreatic head mass. Fine-needle aspiration (FNA) was performed but complicated by post-procedure bleeding and clot formation. The patient denied a personal history of pancreatic disorders but reported parental cancer. Laboratory findings revealed anemia (Hb 9.2 g/dL) and elevated liver function tests (total bilirubin 2.6 mg/dL, AST 146 U/L, ALP 267 U/L, ALT 158 U/L).
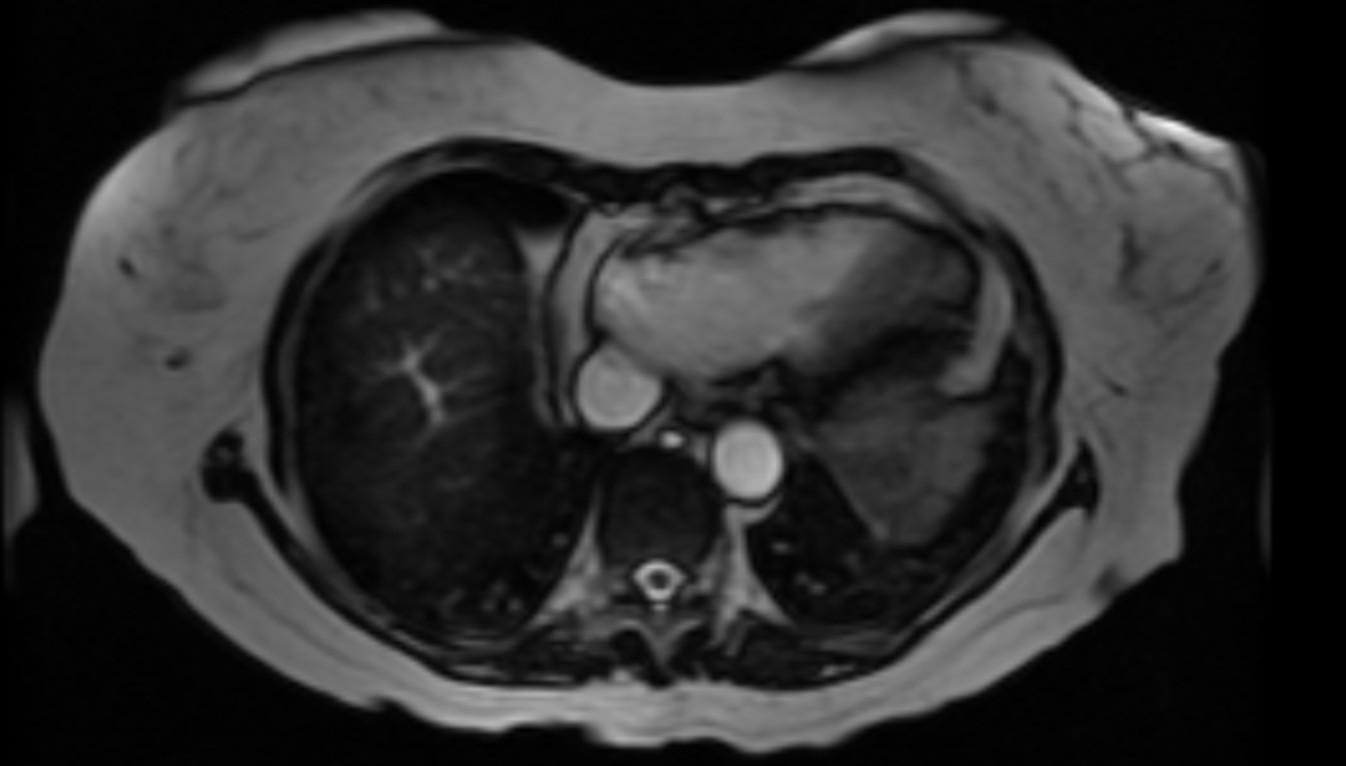
Magnetic resonance cholangiopancreatography (MRCP) showed a centrally necrotic pancreatic mass without ductal dilation. A PET scan demonstrated hypermetabolic lymph nodes in the left upper neck and abdomen. Histopathology of the mass confirmed necrotic DLBCL. The patient was started on Protonix, scheduled for follow-up imaging, and referred for outpatient hepatobiliary surgery consultation. Discussion: Primary pancreatic lymphoma, though rare, should be considered in the differential for pancreatic masses. It typically involves peripancreatic nodes, lacks mediastinal lymphadenopathy, and does not cause main duct dilation. Unlike adenocarcinoma, lymphoma rarely invades vascular structures, making imaging and biopsy crucial for diagnosis.
DLBCL is aggressive and biologically diverse. Management depends on subtype, with germinal center variants responding well to R-CHOP (rituximab, cyclophosphamide, prednisone, doxorubicin, vincristine), while activated B-cell subtypes have worse outcomes. Prognosis is influenced by disease stage, extranodal spread, and lactate dehydrogenase levels.
Considering lymphoma in pancreatic masses ensures early diagnosis. A thorough workup with imaging and biopsy allows for proper treatment, avoids unnecessary surgery, and improves patient outcomes.
Figure: Large abnormal mass in the pancreatic head region, lacking associated hepatic or pancreatic ductal dilatation, identified as necrotic pancreatic lymphoma.
Disclosures: Philip Hall indicated no relevant financial relationships. Vikash Chadive indicated no relevant financial relationships. Harman Sawhney indicated no relevant financial relationships. Taofeek Kolade indicated no relevant financial relationships. Ayesha Samad indicated no relevant financial relationships. Fatima Arslan indicated no relevant financial relationships. Arsalan Ahmad indicated no relevant financial relationships. Shreyas Kunjir indicated no relevant financial relationships. Karim Akl indicated no relevant financial relationships.
Philip Hall, MD, MPH1, Vikash R. Chadive, MBBS2, Harman Sawhney, DO3, Taofeek Kolade, MD1, Ayesha Samad, MD4, Fatima Safi. Arslan, MD1, Arsalan Ahmad, MD1, Shreyas Kunjir, MD5, Karim Akl, MD6. P2331 - Deceptive Mass: The Hidden Threat of Necrotic Pancreatic Lymphoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.