Bobak Moazzami, MD1, Justin Forde, MD2, Tanna Lim, MD2 1Northside Hospital Gwinnett, Atlanta, GA; 2Northside Hospital Gwinnett, Lawrenceville, GA Introduction: Mirizzi syndrome and cholangiocarcinoma are two distinct causes of biliary obstruction that can present with overlapping clinical and radiologic features, often making early diagnosis challenging. The presence of gallstones often leads to an initial assumption of a benign etiology; however, such findings should not exclude the possibility of an underlying malignancy. We present a case initially suspected to be Mirizzi syndrome that was ultimately diagnosed as distal cholangiocarcinoma and later found to be associated with Lynch syndrome.
Case Description/
Methods: A 68-year-old male with a history of diabetes, hyperlipidemia, and bipolar disorder presented with progressive jaundice, pruritus, dark urine, and pale stools. Laboratory workup revealed a cholestatic pattern of liver injury with elevated total bilirubin (11.5 mg/dL), ALT (942 U/L), AST (501 U/L), and CA 19-9 (40 U/mL). Imaging showed cholelithiasis and a 1.4 cm mass at the junction of the cystic and common hepatic ducts, initially raising concern for Mirizzi syndrome. ERCP revealed a compressive cystic duct stone with biliary sludge. Due to persistent obstruction, repeat ERCP with SpyGlass cholangioscopy was performed, revealing a distal biliary stricture. Biopsies confirmed invasive adenocarcinoma of the common hepatic duct. Tumor molecular profiling revealed microsatellite instability-high (MSI-H) status and pathogenic mutations in PMS2 and MSH3, suggestive of Lynch syndrome. PET/CT showed no evidence of metastatic disease. The patient was referred for neoadjuvant chemotherapy followed by planned Whipple resection. Discussion: This case emphasizes the importance of maintaining a high index of suspicion for malignancy in cases of persistent biliary obstruction in presence of Mirrizi syndrome. Advanced endoscopic techniques such as SpyGlass cholangioscopy can aid in timely diagnosis. This case also highlights a rare presentation of cholangiocarcinoma potentially associated with Lynch syndrome, supporting the need for molecular evaluation in select patients.
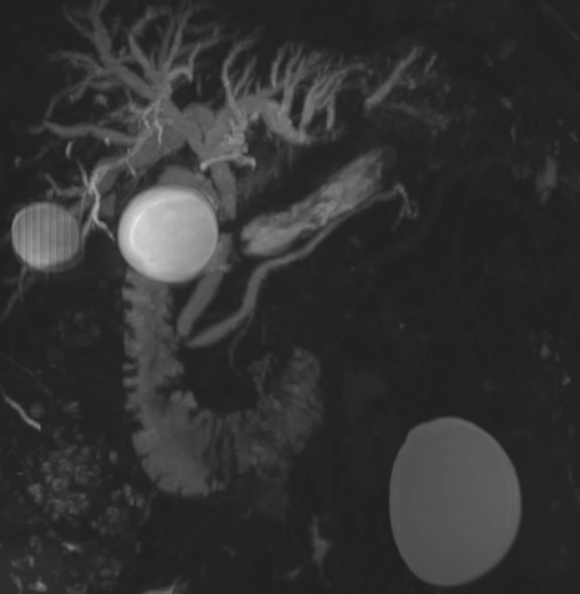
Figure: Magnetic resonance cholangiopancreatography (MRCP) demonstrating intrahepatic biliary ductal dilation with abrupt narrowing at the level of the common bile duct, initially suggestive of Mirizzi syndrome.
Figure: SpyGlass cholangioscopic image revealing a friable, irregular stricture in the distal common bile duct. Biopsies obtained from this site confirmed invasive adenocarcinoma.
Disclosures: Bobak Moazzami indicated no relevant financial relationships. Justin Forde indicated no relevant financial relationships. Tanna Lim indicated no relevant financial relationships.
Bobak Moazzami, MD1, Justin Forde, MD2, Tanna Lim, MD2. P2305 - From Mirizzi to Malignancy: A Case of Lynch Syndrome-Associated Distal Cholangiocarcinoma Masquerading as Mirizzi Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.