Lauren Healey, DO1, Hobie L. Hughes, DO2, William C. Gannaway, BS3, William Sonnier, MD3, Katherine Glosemeyer, MD1 1University of South Alabama, Mobile, AL; 2Thomas Hospital, Fairhope, AL; 3University of South Alabama College of Medicine, Mobile, AL Introduction: Cytomegalovirus (CMV) typically remains dormant in patients with competent immune systems but has the ability to reactivate if the immune system becomes compromised. In rare cases, CMV will become active in patients with functional immune systems. There is a known association between CMV causing hepatitis, however CMV causing an ampullary mass is extremely rare.
Case Description/
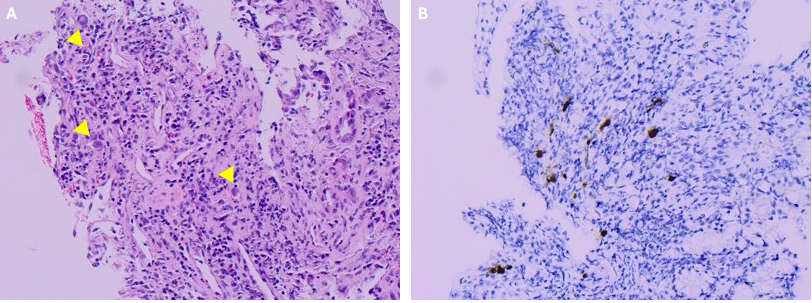
Methods: A 76-year-old male with hypertension but no prior history of immunosuppression presented to the hospital with jaundice, diarrhea, dark brown urine, and right upper quadrant abdominal pain. Labs on admission were significant for leukocytosis, elevated aspartate transaminase and alanine transaminase, elevated alkaline phosphatase, and hyperbilirubinemia. HIV testing was negative. CT of the abdomen and pelvis revealed common bile duct dilation and multiple hepatic hemangiomas that were confirmed with ultrasound. Endoscopic Retrograde Cholangiopancreatography (ERCP) was performed the following day revealing an ampullary mass with ulceration and secondary pyloric stenosis. A biliary drain was placed. The patient developed melena with a drop in Hemoglobin from 10 g/dL to 6.9 g/dL over the next four days requiring transfusion. Esophagogastroduodenoscopy (EGD) did not visualize active bleeding, and cholangiogram showed decreased common bile duct dilation. Ampullary mass biopsies were taken and were positive for CMV with CMV PCR of 109,405 IU/mL. The patient was placed on Ganciclovir and Micafungin, then transitioned to ganciclovir maintenance dose after three weeks. CMV Quant PCR prior to discharge was < 200 IU/mL. The patient was discharged on Ganciclovir as indefinite maintenance therapy. Discussion: CMV infection of the gastrointestinal tract in the form of hepatitis can occur in immunocompromised individuals. Masses of the GI tract caused by CMV are rare in immunocompromised individuals, but extremely rare in an immunocompetent individual. The mechanism of damage caused by CMV is not well-understood and the most accepted hypothesis suggests tissue damage results from activation of cytotoxic T cells against CMV-infected cells.Hepatocytes are most affected, and bile duct cells are rarely involved, as seen in our case. This case emphasizes the importance of considering viral infections in broad differential diagnosis in immunocompetent patients presenting with a mass.
Figure: Figure 2: A single pedunculated ampullary mass
Disclosures: Lauren Healey indicated no relevant financial relationships. Hobie Hughes indicated no relevant financial relationships. William Gannaway indicated no relevant financial relationships. William Sonnier: Abbvie – Speakers Bureau. Eli Lily – Speakers Bureau. Katherine Glosemeyer indicated no relevant financial relationships.
Lauren Healey, DO1, Hobie L. Hughes, DO2, William C. Gannaway, BS3, William Sonnier, MD3, Katherine Glosemeyer, MD1. P2295 - A Rare Case of CMV Presenting as an Ampullary Mass and Cholangitis in an Immunocompetent Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")